The premise sounds implausible. Apply a cuff to your arms or legs, restrict blood flow partially, then train with weights 20 to 30% of your one-rep maximum, and produce muscle growth equivalent to heavy training at 70 to 80% of your maximum.
It sounds like the kind of shortcut that fitness products promise and peer-reviewed research demolishes. In this case, the research supports it. Blood flow restriction training, or BFR, produces hypertrophy comparable to high-load resistance training through a mechanism that does not depend on heavy mechanical loading. The research base is extensive: hundreds of randomised controlled trials, multiple systematic reviews and meta-analyses, and clinical application in rehabilitation settings where the evidence is strongest.
This guide covers the physiological mechanism of BFR, what the meta-analysis evidence shows about its effectiveness compared to conventional training, who the ideal candidates are, how to apply it safely, and practical protocols for different training goals.
The Mechanism: Why Restricting Blood Flow Produces Muscle Growth
What BFR Actually Does Physiologically
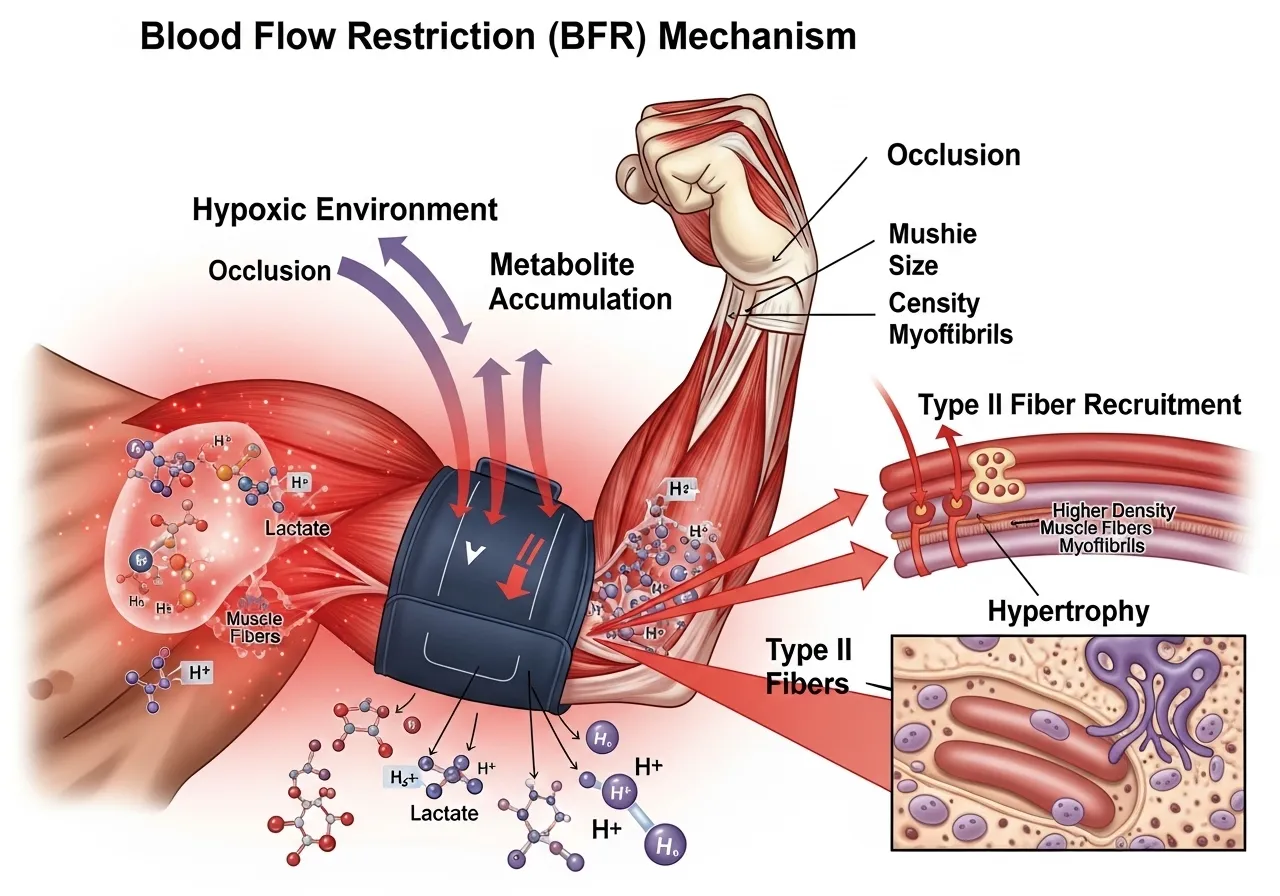
Blood flow restriction training works by applying a cuff or wrap to the proximal portion of a limb, partially restricting venous outflow while allowing arterial inflow to continue at a reduced rate. The result is blood pooling in the working muscle, creating a localised hypoxic environment during exercise.
This hypoxic accumulation triggers multiple hypertrophy-relevant responses simultaneously. Metabolite accumulation, specifically lactate, inorganic phosphate, and hydrogen ions, increases significantly beyond what equivalent-load training without restriction produces. This metabolite environment stimulates growth hormone release, IGF-1 production, and cell swelling that the muscle interprets as a hypertrophic stimulus. The fast-twitch type II fibres, which preferentially fatigue under the hypoxic conditions created by BFR, are recruited earlier in a low-load BFR set than they would be under matched low-load training without restriction. This type II recruitment at low loads is the core mechanism that makes BFR uniquely effective.
What BFR Does Not Do
BFR does not restrict arterial inflow to zero. It is partial venous restriction, not arterial occlusion. The cuff pressure reduces but does not eliminate blood flow, maintaining tissue oxygenation at a level that allows exercise while creating sufficient hypoxic stimulus to trigger the metabolite cascade. Complete arterial occlusion during exercise is dangerous. BFR at appropriate pressures is not.
BFR also does not replace the mechanical tension stimulus of heavy training for strength development. The research consistently shows BFR produces hypertrophy comparable to heavy training but strength gains inferior to heavy training. Maximal strength requires heavy mechanical loading that BFR cannot replicate. BFR is an additional hypertrophy tool that works through a different mechanism than conventional loading, not a complete replacement for heavy resistance training.
The History: From KAATSU to Clinical Practice
Blood flow restriction training originates from Japan, where Yoshiaki Sato developed the KAATSU method in the 1970s after observing that restricted blood flow during prolonged kneeling produced a training-like sensation in his calves. Sato spent years refining the cuff pressure parameters and exercise protocols before the method entered formal scientific study in peer-reviewed journals. The first peer-reviewed research on BFR appeared in Japanese literature in the 1990s and entered the English-language sports science and rehabilitation literature in the early 2000s, gradually accumulating the evidence base that now spans hundreds of randomised controlled trials.
Clinical adoption accelerated in the 2010s as rehabilitation researchers recognised BFR’s potential for post-surgical muscle maintenance. The US military subsequently funded BFR research for injury recovery in soldiers, and the technique became standard in many sports medicine and physical therapy settings. The transition from fringe Japanese strength training method to evidence-supported clinical rehabilitation tool represents one of the more unusual trajectories in modern exercise science. Most of the evidence base now derives from peer-reviewed randomised controlled trials and systematic reviews rather than the informal practitioner observations that characterised BFR’s early research history.
What the Meta-Analysis Evidence Shows: BFR vs High-Load Training
📌 Key Finding
BFR training produces equivalent muscle hypertrophy to high-load resistance training at 20 to 30% 1RM versus 70 to 80% 1RM. Strength gains favour high-load training (SMD -0.33). For hypertrophy goals specifically, BFR achieves the same outcome with a fraction of the mechanical joint loading.
Moderating Factors: What Affects BFR Effectiveness
📌 Key Finding
BFR effectiveness varies by population, limb, and protocol. Lower limb BFR generally produces stronger effects than upper limb BFR. Untrained individuals show larger relative gains from BFR than trained individuals. Protocol variables including frequency and duration meaningfully affect outcomes.
📌 Key Finding
BFR produces significantly greater muscle gains than low-load training without restriction in older adults (SMD 0.51 for hypertrophy). For older trainees who cannot safely use high loads, BFR provides a hypertrophy stimulus that conventional light-weight training cannot match.
Is BFR Training Right for You? Who Benefits and Who Should Avoid It
The Ideal BFR Candidates
BFR training is not a universally superior alternative to conventional training. It is a specific tool that solves specific problems. The trainees who benefit most share a common characteristic: they need hypertrophy or strength maintenance stimulus but cannot or should not use the heavy loads that conventional training requires.
Post-surgical rehabilitation: The earliest and most evidence-supported use of BFR. After knee reconstruction, hip replacement, or rotator cuff repair, high mechanical loads are contraindicated but muscle atrophy begins immediately. BFR at 20 to 30% 1RM provides hypertrophy stimulus without joint loading stress, maintaining muscle mass during the healing period.
Older adults: Joint sensitivity and connective tissue limitations frequently prevent older trainees from tolerating high loads. BFR provides the hypertrophy stimulus that maintains lean mass and functional strength with loads the joints can manage.
Injury-modified training: Trainees with active tendinopathy, stress fractures, or acute muscle strains can often train the uninjured portion of the body normally while using BFR for the injured limb at loads the injury tolerates.
High-volume athletes managing joint load: Elite strength and endurance athletes use BFR at the end of training blocks when accumulated joint fatigue makes high-load training inadvisable, maintaining muscle stimulus during deload periods.
Who Should Not Use BFR
⚠️ BFR Contraindications Blood flow restriction training is contraindicated for individuals with cardiovascular disease, hypertension above 160/100 mmHg, deep vein thrombosis history or active DVT risk, varicose veins at the cuff application site, peripheral arterial disease, lymphoedema, sickle cell trait, pregnancy, or open wounds at the cuff application site. BFR should not be applied to the trunk or neck. Anyone with a history of blood clotting disorders should obtain medical clearance before beginning BFR training.
BFR for Recreational Trainees Without Injury
Healthy recreational trainees without injury limitations benefit from BFR primarily as a supplement to conventional training rather than a replacement. Adding 1 to 2 BFR sessions per week as finishing work after primary heavy training provides additional hypertrophy volume at low fatigue cost. The lighter loads used in BFR sessions do not significantly impair recovery from conventional training, allowing total weekly volume to increase without proportional fatigue accumulation.
The practical application for recreational trainees: at the end of a leg session, after completing conventional squats and deadlifts, apply a thigh cuff and perform 4 sets of leg extensions at 25% of 1RM using the 30-15-15-15 protocol. The metabolite accumulation after heavy compound work may be amplified by the pre-fatigue from conventional training, potentially increasing the BFR stimulus beyond what the same protocol would produce on fresh legs. This sequencing means BFR adds volume without adding session time beyond the cuff application and a few sets at very light load.
For upper body, a similar approach works with bicep curl or tricep pushdown BFR after heavy rowing and pressing. Trainees who have hit a plateau in arm development despite consistent training often find BFR creates a novel stimulus that conventional training cannot produce at the same total joint load. The bodyweight training approach that complements light-load training methods is covered in the bodyweight training guide.
How to Apply BFR: Cuff Pressure, Load, Volume, and the Practical Variables
Cuff Pressure: The Most Critical Variable
The cuff pressure determines whether BFR training is safe and effective or simply uncomfortable and counterproductive. Pressure is expressed as a percentage of limb occlusion pressure (LOP), which is the minimum pressure needed to completely stop arterial blood flow in the limb at rest.
The evidence-based pressure range is 40 to 80% of LOP for lower limb BFR and 40 to 50% of LOP for upper limb BFR. These pressures produce adequate venous restriction without arterial occlusion. Using fixed absolute pressures rather than LOP percentages is less accurate because limb circumference, muscle mass, and cardiovascular factors all affect how much pressure is needed for each individual.
Without access to a Doppler ultrasound device to measure LOP precisely, a practical approximation for lower limb BFR: apply the cuff to the upper thigh at a tightness of 6 to 7 out of 10, where the limb feels moderately tight but not painful and the skin distal to the cuff does not turn pale or purple. For upper limb BFR on the upper arm: 5 to 6 out of 10 tightness. These are starting points that should be adjusted based on the sensation during training, not fixed prescriptions.
Load, Volume, and Rest: The Standard BFR Protocol
Load: 20 to 30% of 1RM. At this load without restriction, 50 to 100 reps could be performed. With BFR restriction, fatigue occurs within 15 to 30 reps due to the hypoxic environment. Set structure: 1 set of 30 reps followed by 3 sets of 15 reps (the 30-15-15-15 protocol). Total of 75 reps per exercise. Rest between sets: 30 to 45 seconds with the cuff remaining inflated. Short rest periods are critical: removing or deflating the cuff between sets allows the metabolite accumulation to dissipate and reduces the hypoxic stimulus. Cuff duration: Maximum 5 to 6 minutes of continuous cuff inflation per exercise. Deflate completely between exercises.
Exercise Selection for BFR
BFR works best with single-joint or simple compound exercises where the cuff can be applied to the proximal limb segment effectively. Leg extensions, leg curls, knee extensions, bicep curls, and tricep pushdowns are the most commonly studied and applied BFR exercises. Multi-joint exercises requiring complex coordination, such as squats or deadlifts, are less effective for BFR because the cuff positioning is less precise and the movement pattern is harder to maintain during the cognitive distraction of cuff discomfort.
The resistance band training framework and how it relates to BFR’s variable resistance profile is covered in the resistance bands guide.
Pacing and Effort Within BFR Sets
BFR sets feel distinctly different from conventional training sets. The metabolite accumulation produces a burning sensation within the first 10 to 15 reps that intensifies progressively through the set. This is the mechanism working. Stopping early because the burning feels uncomfortable defeats the purpose of BFR. Sets should be taken close to muscular failure, as the metabolite stimulus is greatest in the final reps when accumulation peaks.
The 30 to 45 second rest periods between sets are deliberately short. Longer rest periods allow metabolite clearance that reduces the next set’s stimulus. If short rest periods make maintaining the 15-rep target difficult, the cuff pressure may be too high or the load too heavy. Adjust only one variable at a time: first reduce cuff tightness slightly and reassess for two sessions, then reduce load if the problem still persists.
Monitoring Sensations During BFR
Certain sensations during BFR training require stopping immediately. Numbness or tingling in the digits distal to the cuff suggests the pressure restricts arterial flow too aggressively. Pale or blue-white skin distal to the cuff indicates arterial occlusion and requires immediate cuff removal. Dizziness after cuff removal is common and typically resolves within 60 seconds. Simply sitting down for 60 to 90 seconds after session completion reduces this risk substantially.
Normal BFR sensations include a tight pressured feeling at the cuff site, intense burning in the muscle during sets, significant fatigue within 20 to 30 reps, and a pronounced pump effect persisting for 5 to 15 minutes post-session. These sensations confirm the mechanism is working and require no action beyond completing the planned sets and deflating the cuff as scheduled.
📅 Phase 1: Weeks 1 to 2: Pressure Calibration and Tolerance
2 sessions per week
Lower limb only: leg extension or leg curl with thigh cuff
Load: 20% estimated 1RM
Sets: 1 × 30 reps, then 2 × 15 reps (remove cuff between exercises, not between sets)
Goal: identify correct cuff tightness, assess tolerance, note any discomfort beyond normal fatigue
The cuff sensation is unusual. The first two weeks are about calibration and adaptation to the restriction, not training stimulus optimisation.
📅 Phase 2: Weeks 3 to 4: Full Protocol
2 to 3 sessions per week
Add upper limb BFR if desired: bicep curl or tricep pushdown with upper arm cuff
Full 30-15-15-15 set structure for each exercise
Load: 20 to 30% 1RM, rest 30 to 45 seconds between sets with cuff inflated
Perform BFR as finisher after primary conventional training, not as primary workout
BFR after conventional training when the muscle is already partially fatigued may enhance the metabolite accumulation effect. Adjust cuff pressure if any numbness, tingling, or discolouration appears during sets.
Combining BFR With Conventional Training
The most effective use of BFR for general fitness trainees is as a supplement to primary conventional training, not a replacement. Perform 3 to 4 conventional sets of a movement, then apply BFR for 1 to 2 finishing sets at 20 to 30% load. This provides both the mechanical tension stimulus of heavy loading and the metabolite-mediated stimulus of BFR within the same session. The isometric training research on how sustained contractions relate to the metabolite accumulation of BFR is covered in the isometric training guide.
BFR for Walking: The Older Adult Application
One of the most evidence-supported applications of BFR is adding a cuff to the thighs during slow walking. BFR walking at 40 to 60% of limb occlusion pressure produces measurable increases in quadriceps and hamstring cross-sectional area in older adults who cannot tolerate the loads required for conventional resistance training hypertrophy. The walking speed and intensity is essentially normal walking speed, making the intervention accessible to individuals with significant physical limitations.
For older adults whose primary goal is preserving lower body muscle mass and functional strength for activities of daily living, BFR walking represents a low-barrier entry to the muscle stimulus that prevents the sarcopenic muscle loss accelerating frailty. Two to three sessions per week of 10 to 15 minutes of BFR walking at comfortable pace produces meaningful quadriceps hypertrophy within 8 to 12 weeks in previously sedentary older individuals. The physiological basis for this response is the same metabolite accumulation mechanism that produces hypertrophy in resistance-trained athletes at heavy loads: the restriction creates a hypoxic environment that recruits type II muscle fibres during an activity that would otherwise provide no meaningful muscle stimulus whatsoever. This low-barrier application makes BFR walking one of the most practically accessible tools for maintaining lower body muscle mass in older adults who lack access to a fully equipped gym or who cannot tolerate the mechanical demands of conventional resistance training loads on aging joints.
Frequently Asked Questions About Blood Flow Restriction Training
Is BFR training safe?
BFR training at appropriate pressures and in healthy individuals without the contraindications listed above is well-supported as safe by a substantial body of clinical research. The most common adverse effects are mild: temporary bruising at the cuff site, delayed onset muscle soreness more intense than conventional training, and lightheadedness in some individuals immediately after cuff removal. These effects are transient and do not represent injury.
Serious adverse events from BFR training in healthy populations are rare in the research literature. Research documents isolated DVT events in individual case reports, which is why DVT history and risk factors stand as absolute contraindications. At supervised clinical pressures, BFR does not increase rhabdomyolysis risk or cause nerve damage in healthy individuals.
What equipment do I need for BFR?
Dedicated BFR cuffs, either pneumatic (air-filled with a pressure gauge) or elastic wraps, are the primary equipment requirement. Pneumatic cuffs with a gauge allow consistent pressure measurement and are preferred for clinical applications and for trainees who want precise, repeatable pressure across sessions. Elastic wraps are less expensive and more portable but cannot be calibrated to a specific pressure percentage, requiring subjective tightness assessment instead.
Generic knee wraps or blood pressure cuffs are not ideal substitutes. Knee wraps apply uneven pressure and lack width adequate to restrict the correct vessel anatomy. Blood pressure cuffs are not designed for the pressure ranges and movement demands of BFR exercise. Dedicated BFR products from established manufacturers are the appropriate starting point for trainees committing to regular BFR training.
Does BFR training hurt?
BFR training is genuinely uncomfortable. The cuff creates sustained pressure at the application site and the metabolite accumulation during sets produces an intense burning sensation that is considerably more pronounced than equivalent-load conventional training without restriction. Most trainees rate BFR sets at 7 to 9 out of 10 perceived exertion despite the very light absolute loads used, because the restriction creates an internal environment that makes light weights feel genuinely taxing.
This discomfort is the training mechanism, not a warning sign. The burning sensation from metabolite accumulation in the restricted limb is what drives the hypertrophy response. Trainees who find the discomfort too severe at full cuff pressure can reduce cuff tightness slightly and reassess. Starting at the lower end of the recommended pressure range allows tolerance to develop over two to four weeks before progressing toward standard BFR pressures.
Can BFR training cause blood clots?
The risk of deep vein thrombosis from BFR training in healthy individuals without DVT risk factors is very low based on current research. BFR uses partial venous restriction, not complete occlusion, and the exercise itself maintains venous return through muscular pumping during contractions. DVT formation requires prolonged venous stasis, which complete limb immobilisation produces but BFR exercise does not.
The caution around DVT history as a contraindication is appropriate because individuals who have previously formed clots have elevated baseline DVT risk. For the general healthy population, BFR training does not elevate DVT risk meaningfully above baseline. The cardiovascular risk with BFR is more accurately characterised as acute blood pressure elevation and increased cardiac workload during the restricted session, which is why cardiovascular disease and uncontrolled hypertension are the primary contraindications.
How quickly does BFR produce results?
Measurable muscle cross-sectional area increases from BFR training appear within 4 to 8 weeks of consistent training. This timeline is comparable to conventional resistance training hypertrophy response rates. Strength improvements from BFR appear more slowly than hypertrophy improvements and plateau below the strength gains achievable with equivalent-volume high-load training.
For rehabilitation applications, the muscle maintenance benefit of BFR appears within the first 2 to 3 weeks: BFR-trained post-surgical limbs show significantly less atrophy compared to untreated limbs in trials of similar duration. This early atrophy prevention effect is arguably the most clinically significant benefit of BFR, producing meaningful functional outcome differences even in short rehabilitation windows. The bodyweight training progression that complements BFR rehabilitation work is covered in the bodyweight training guide.
Key Takeaways
BFR training produces equivalent muscle hypertrophy to high-load resistance training at 20 to 30% 1RM by creating a hypoxic metabolite environment that stimulates type II fibre recruitment at loads that would normally not achieve it.
Strength gains favour high-load training (SMD -0.33). For trainees whose primary goal is hypertrophy and who cannot use heavy loads, BFR achieves equivalent outcomes with a fraction of the joint loading.
BFR is superior to conventional low-load training without restriction in older adults (SMD 0.51 for hypertrophy), making it the most evidence-supported tool for muscle maintenance in populations where heavy loading is contraindicated.
Cuff pressure of 40 to 80% of limb occlusion pressure for lower limbs and 40 to 50% for upper limbs. The 30-15-15-15 set structure with 30 to 45 second rest between sets and cuff remaining inflated is the standard evidence-based protocol.
BFR is contraindicated with cardiovascular disease, DVT history, hypertension above 160/100, peripheral arterial disease, and several other conditions. Obtain medical clearance before starting BFR if any contraindication applies.
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. Resistance Bands: The $30 Training Tool That Belongs in Every Serious…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…
⚠️ Shoulder, Spine, and Core Safety NoteLandmine exercises involve rotational and asymmetric loading that stresses the shoulder in an oblique pressing pattern and the lumbar spine in lateral and rotational planes. Individuals with active shoulder impingement, rotator cuff tears, lumbar disc herniation, or diagnosed spinal instability should obtain medical clearance before landmine training. During rotation-based…
Walk into any gym and you will find cable stacks, pull-up bars, and Smith machines. Gymnastic rings are the one piece of equipment almost nobody uses. They also happen to be the one piece that trains the quality every other tool ignores: three-dimensional shoulder stability under dynamic load. Rings hang freely. They rotate, swing, and…
Why TRX training overview and Suspension Training Belong in Every Serious Training Program The TRX suspension trainer — two adjustable straps with handles anchored to a single point, allowing the exerciser to use their own bodyweight and gravity as resistance through an infinite range of angles and positions — has earned a permanent place in…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only and does not replace professional medical advice. If you have any lower limb, knee, or ankle conditions, please consult a qualified healthcare professional before beginning plyometric training overview training. Plyometric training — exercise that uses the stretch-shortening cycle (the rapid lengthening of a…


")










