Why Shoulder Mobility Is the Foundation of Pain-Free Upper Body Training
The shoulder is the most mobile joint in the human body — capable of movement in more planes and across greater ranges than any other major joint. This exceptional mobility comes at the cost of inherent instability: the glenohumeral joint’s ball-and-socket architecture allows enormous range of motion but requires the surrounding musculature to actively stabilize the humeral head in the glenoid throughout every movement. When the muscles that control shoulder mobility — the rotator cuff, scapular stabilizers, and thoracic extensors — are insufficient or imbalanced, the exceptional mobility that makes the shoulder so functional becomes the source of the impingement, instability, and pain that affects an estimated twenty-six percent of adults at any given time.
Most shoulder pain and mobility restriction that recreational athletes experience is not structural — not rotator cuff tears, not significant labral damage, not bony abnormalities — but functional: the consequence of the muscular imbalances, postural adaptations, and mobility restrictions that modern life and pressing-dominant training systematically create. Anterior shoulder tightness from prolonged sitting and bench pressing, thoracic kyphosis from desk work, and weak posterior rotator cuff from neglected external rotation training combine to produce the rounded shoulder posture and restricted overhead mobility that most adults accept as normal and inevitable. They are neither.
The Three Primary Sources of Shoulder Mobility Restriction
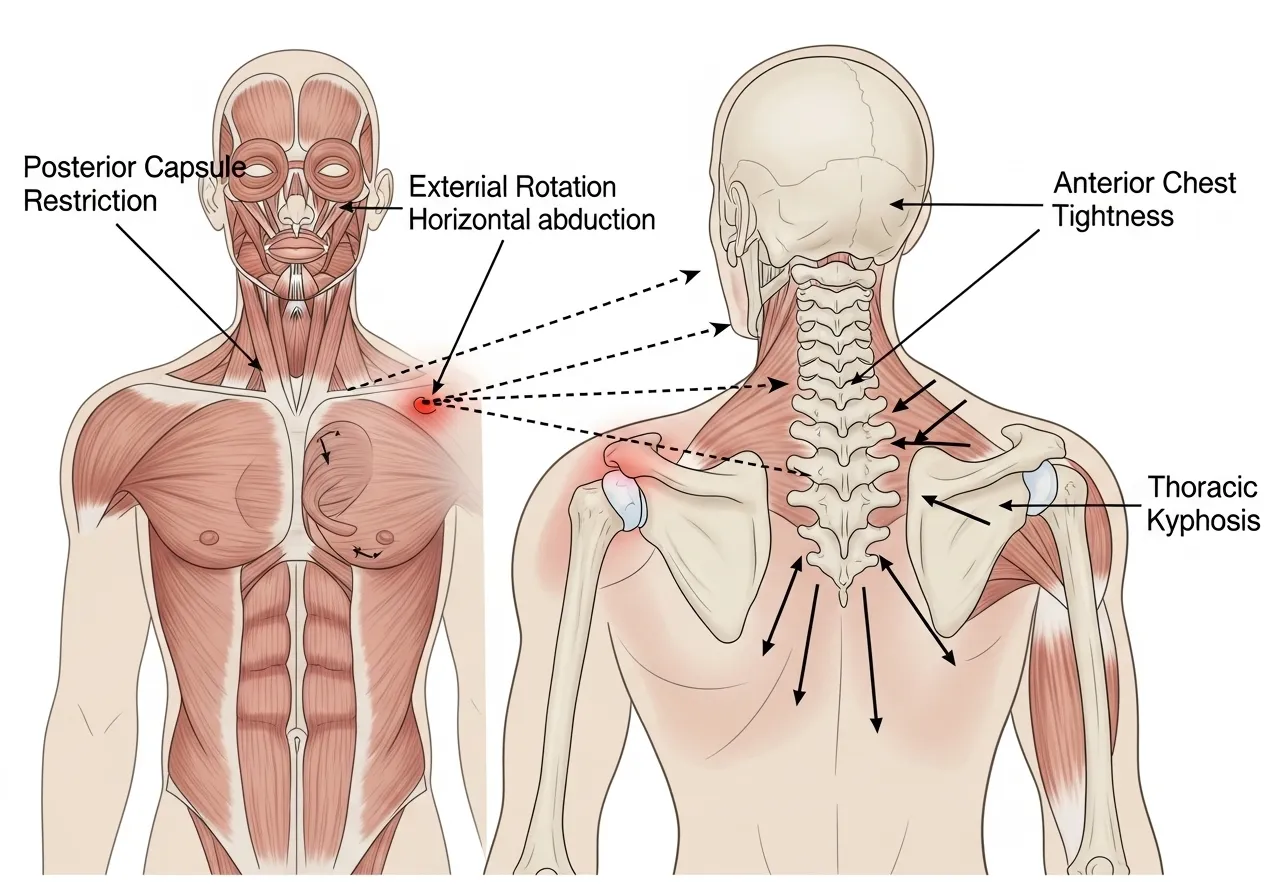
Posterior capsule tightness — restriction of the posterior glenohumeral joint capsule — limits the shoulder’s ability to internally rotate and cross the body, producing the impingement that causes anterior shoulder pain during pressing and overhead movements. Anterior chest tightness — shortening of the pectoralis minor and major — pulls the scapula into protraction and the humerus into internal rotation, reducing the subacromial space and creating impingement risk during elevation. Thoracic kyphosis — excessive rounding of the upper back — prevents the scapula from rotating upward fully during arm elevation, mechanically blocking overhead range of motion regardless of shoulder-specific mobility. Research on shoulder impingement consistently identifies all three as primary modifiable contributors, and the mobility program described in this article addresses all three simultaneously. According to NCBI research on regional interdependence and shoulder function, thoracic spine mobility significantly affects shoulder elevation mechanics, confirming that shoulder mobility programs must address the thoracic spine alongside the shoulder joint itself.
Action point: Perform this simple shoulder mobility screen: stand against a wall with your feet six inches from the wall, lower back flat, and try to raise both arms overhead until your wrists touch the wall above your head. If your lower back arches away from the wall, your elbows bend significantly, or you cannot reach the wall, you have meaningful shoulder mobility restriction that the program in this article directly addresses.
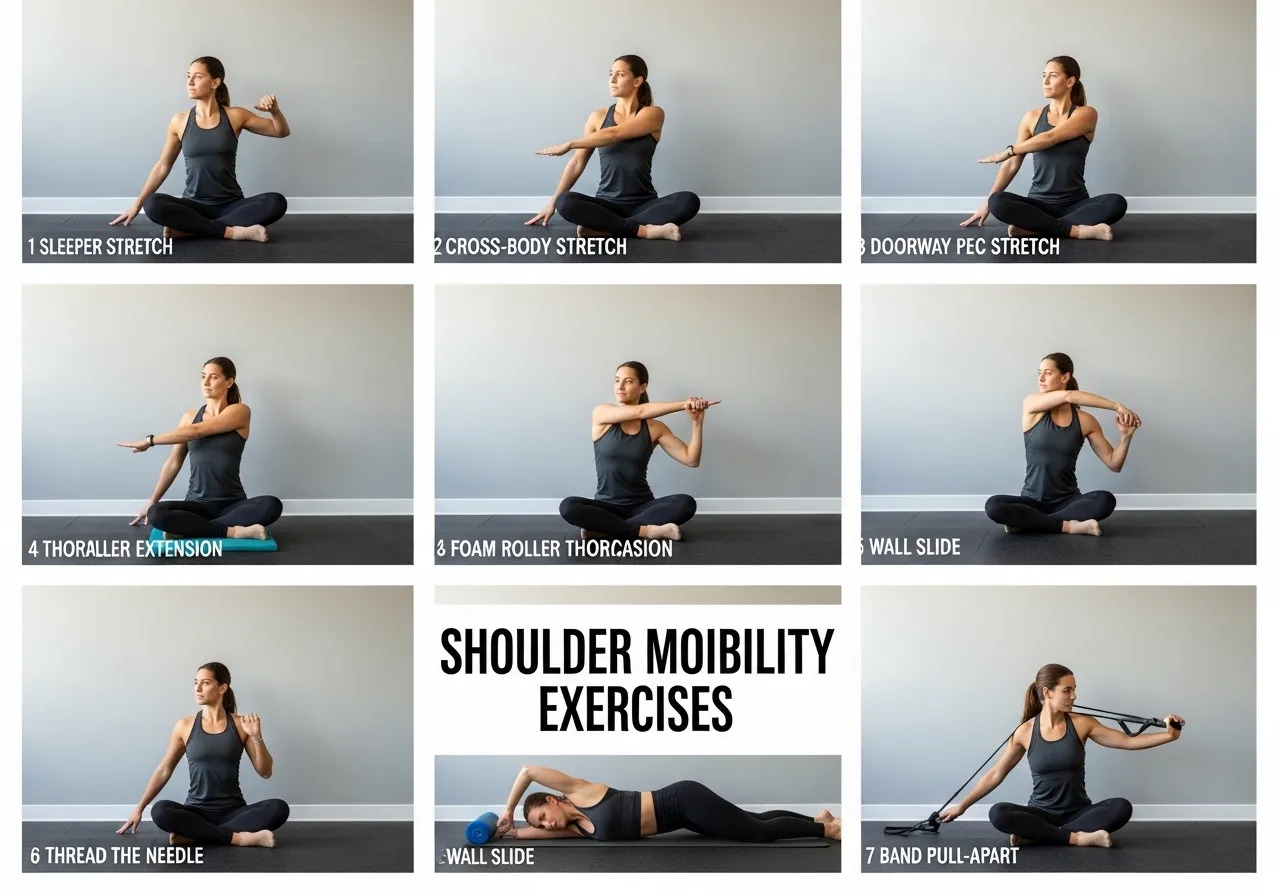
The Seven Essential Shoulder Mobility Exercises
The following exercises address all three primary sources of shoulder mobility restriction — posterior capsule tightness, anterior chest tightness, and thoracic kyphosis — in a sequence that progressively opens the shoulder complex from its foundational restrictions through to functional overhead range of motion.
Exercise 1: Sleeper Stretch (Posterior Capsule)
Lie on your side with the bottom shoulder at 90 degrees of abduction and the elbow bent to 90 degrees. Using the top hand, gently press the bottom forearm toward the floor (increasing internal rotation) until a stretch is felt in the posterior shoulder. Hold for 30 seconds, relax, repeat three times per side. The sleeper stretch is the most evidence-supported posterior capsule mobilization for shoulder impingement rehabilitation. Research comparing capsule stretching techniques consistently finds the sleeper stretch produces superior posterior capsule length improvements compared to other commonly prescribed posterior shoulder stretches. According to research on posterior capsule stretching and shoulder impingement, the sleeper stretch produces significant improvements in shoulder internal rotation range and reductions in impingement symptoms within four to six weeks of consistent daily practice.
Standing or seated, bring one arm across the body at shoulder height and use the opposite hand to pull the arm gently closer to the chest. Hold for 30 seconds per side. This targets the posterior capsule and posterior deltoid, complementing the sleeper stretch by loading the posterior structures in a different position. Perform three repetitions per side daily.
Stand in a doorway with both arms against the door frame at 90 degrees of abduction and 90 degrees of elbow flexion. Step forward until a stretch is felt across the chest. Hold for 30 seconds, relax, repeat three times. This targets the pectoralis major and minor, reversing the anterior shortening that pressing dominance and prolonged sitting create. A variation with the arms higher (approximately 120 degrees of abduction) targets the upper pectoralis and coracoclavicular structures.
Exercise 4: Foam Roller Thoracic Extension
Place a foam roller perpendicular to the spine at approximately mid-thoracic level (T6-T8). Support the head with interlaced hands and gently extend the thoracic spine over the roller, allowing gravity to create extension. Hold each position for 30-60 seconds and move the roller to three to four positions along the mid and upper thoracic spine. This addresses thoracic kyphosis — the postural restriction that mechanically limits overhead shoulder elevation regardless of shoulder-specific mobility work.
Exercise 5: Thread-the-Needle Thoracic Rotation
From quadruped (hands and knees) position, slide one arm under the body as far as possible while allowing the thoracic spine to rotate, then reach that arm as high overhead as possible on the opposite side. Ten repetitions per side develops thoracic rotation mobility that is essential for overhead movements in asymmetrical sport activities and daily reaching tasks.
Exercise 6: Wall Slide
Stand with your back against a wall, feet six inches from the wall, and lower back flat against the wall. Place both arms against the wall at 90 degrees of abduction and 90 degrees of elbow flexion (“goalpost” position). Slowly slide the arms overhead while maintaining full contact of the forearms and wrists with the wall. Ten repetitions of this exercise simultaneously stretches the pectorals and lats while activating the lower trapezius and serratus anterior — the scapular stabilizers most commonly weakened in people with restricted overhead mobility.
Exercise 7: Band Pull-Apart
Hold a resistance band at shoulder height with arms extended. Pull the band apart until the hands are beside the shoulders, squeezing the shoulder blades together and activating the posterior deltoids and external rotators. Three sets of fifteen repetitions daily develops the posterior shoulder chain strength that counters anterior dominance and creates the stable shoulder girdle that overhead mobility requires to be functionally usable under load.
Action point: Perform this complete seven-exercise sequence daily for four weeks before reassessing the wall overhead test described in the previous section. Most people see measurable overhead range improvement within two weeks and dramatic improvement within four weeks of daily practice.
The seven exercises in this program are not arbitrary selections — each addresses a specific restriction pattern that the most common sources of shoulder mobility limitation produce, and each produces the specific adaptation that resolves that pattern most efficiently. Performing them daily, with the quality of attention that produces genuine range improvement rather than merely the appearance of exercise, transforms shoulder function in the weeks and months that consistent practice enables.
Shoulder Mobility for Specific Training Activities
Different training activities create specific shoulder mobility demands and specific restriction patterns. Understanding which mobility limitations are most relevant to your primary training activities allows targeted intervention that produces the performance improvements most directly relevant to how you train.
Shoulder Mobility for Overhead Pressing
Overhead pressing — barbell and dumbbell overhead press, push press, handstand push-up — requires full shoulder flexion (arm overhead) combined with thoracic extension and scapular upward rotation. The most common limiting factors: thoracic kyphosis that mechanically blocks full overhead elevation by preventing the scapula from rotating upward, and anterior shoulder tightness that forces the arm to travel forward of vertical at full elevation. The specific mobility work most important for overhead pressing: daily foam roller thoracic extension (three to four positions, 60 seconds each), wall slides (three sets of ten), and band pull-aparts (three sets of fifteen). Athletes who address thoracic mobility and anterior shoulder tightness before attempting to force heavier overhead pressing typically find their press limit increases by five to fifteen percent within four to six weeks — not from additional strength training but from removing the mobility restriction that was preventing existing strength from being expressed in the overhead position.
Shoulder Mobility for Bench Pressing
Bench pressing requires external rotation capacity and posterior capsule flexibility — the ability of the shoulder to move into the externally rotated, horizontally abducted position without anterior impingement or pain. The most common shoulder problem in heavy bench pressers is anterior shoulder impingement from posterior capsule tightness that forces the humeral head forward in the glenoid during the eccentric phase. Daily sleeper stretch and cross-body stretch address posterior capsule tightness specifically, while the face pull and band pull-apart exercises develop the external rotation strength that counters the internal rotation load of bench pressing. Research on shoulder health in powerlifters consistently identifies posterior capsule tightness as the primary modifiable risk factor for bench press-related shoulder injury. According to research on shoulder impingement in powerlifters, daily posterior capsule stretching reduces bench press-related shoulder pain incidence by up to sixty percent in athletes with diagnosed posterior tightness.
Shoulder Mobility for Swimming and Overhead Sports
Swimming — particularly freestyle and butterfly — requires extreme shoulder internal rotation during the pull phase and external rotation during recovery. Volleyball spiking, tennis serving, and baseball throwing require external rotation range that exceeds the general population average. These populations have opposite mobility needs from most gym-based athletes: where gym athletes need more external rotation capacity and posterior capsule length, overhead sport athletes often need anterior capsule flexibility (more horizontal abduction and external rotation range) and posterior shoulder strength to decelerate the throwing arm. Overhead sport athletes benefit from the band pull-apart and sleeper stretch exercises in this program but should supplement with anterior capsule stretching (horizontal abduction stretch against a wall or doorframe) and eccentric external rotation strengthening to address the specific demands their sport creates.
Action point: Identify your primary training activity and review which specific mobility limitations most affect its performance. Prioritize the two to three exercises from the seven-exercise program that most directly address your activity-specific restrictions, performing these daily rather than the complete sequence when time is limited.
Shoulder Mobility Assessment: Understanding What Is Actually Limiting You
Effective shoulder mobility improvement requires identifying which specific restriction is present rather than applying generic shoulder mobility work that may not address the actual limiting factor. Three simple assessments reveal the primary source of restriction and guide targeted intervention.
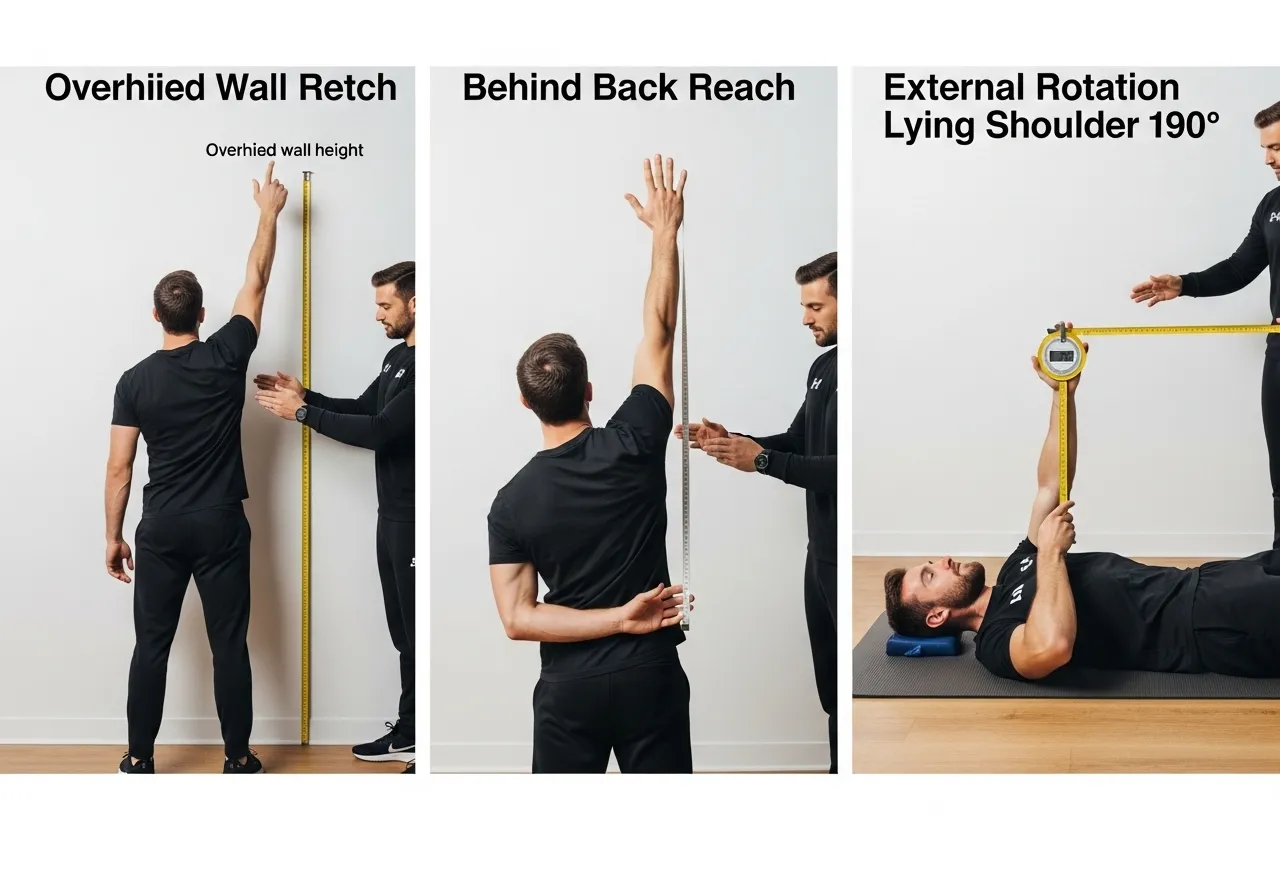
Assessment 1: Overhead Reach Test
Stand against a wall as described in the introduction. If you cannot reach overhead without lower back arching or elbow bending, determine whether the restriction is thoracic (the lower back arches significantly suggesting thoracic kyphosis is the primary limiter) or glenohumeral (the back stays flat but the arms stop short of the wall suggesting shoulder-specific restriction). Thoracic restriction responds to foam roller extension and thoracic rotation work; glenohumeral restriction responds to sleeper stretch, cross-body stretch, and pectoral stretching.
Assessment 2: Internal Rotation Behind-Back Test
Reach one hand up the back from below (as if scratching between the shoulder blades from the bottom) and note how high the thumb reaches. A thumb reaching to T7 or higher indicates adequate internal rotation; a thumb reaching only to the lumbar region indicates posterior capsule tightness requiring sleeper stretch intervention. Compare both sides — asymmetry greater than two vertebral levels suggests posterior capsule tightness on the restricted side that may contribute to impingement during pressing and throwing activities.
Assessment 3: External Rotation Test
Lie on your back with the upper arm at 90 degrees of abduction and the elbow bent to 90 degrees. Allow gravity to lower the forearm toward the floor (external rotation). If the forearm stops significantly before reaching the floor (more than 15-20 degrees from horizontal), external rotation restriction is present — typically from anterior capsule tightness or subscapularis shortening. This restriction is most relevant for overhead sport athletes and for pressing athletes who notice anterior shoulder pain during the bottom position of overhead pressing.
Using Assessment Results to Prioritize Mobility Work
Based on assessment results: primarily thoracic restriction — prioritize foam roller extension, thread-the-needle, and wall slides; primarily posterior capsule restriction — prioritize sleeper stretch, cross-body stretch, and face pulls; primarily anterior restriction — prioritize doorway pectoral stretch, horizontal abduction stretching, and band pull-aparts. Re-assess every four weeks to confirm that the targeted work is producing measurable improvement. If an assessment shows no improvement after four weeks of daily targeted work, professional evaluation from a physical therapist or sports medicine physician is warranted to determine whether structural factors require different treatment approaches. According to Journal of Orthopaedic and Sports Physical Therapy guidelines, systematic mobility assessment before and during intervention programs produces superior outcomes compared to generic mobility programs applied without individual assessment.
Action point: Perform all three assessments before beginning the mobility program and record the results with measurements where possible (thumb height in the behind-back test, degrees of forearm elevation in the external rotation test). Reassess at four and eight weeks to confirm progress and adjust the program emphasis based on which restrictions are resolving and which require continued targeted work.
The Relationship Between Thoracic Mobility and Shoulder Function
The thoracic spine’s mobility — specifically its ability to extend and rotate — is one of the primary determinants of shoulder overhead function, yet it is rarely addressed in programs that focus exclusively on shoulder-specific exercises. The mechanical relationship is direct: scapular upward rotation, which allows the humeral head to clear the acromion during arm elevation, requires the thoracic spine to extend as the arm rises overhead. A thoracic spine locked in flexion (kyphosis) mechanically prevents the scapula from rotating upward fully, creating subacromial impingement at arm elevations above 90 degrees regardless of how much shoulder-specific mobility work is performed. This regional interdependence — where thoracic restriction produces shoulder symptoms — explains why many athletes with shoulder pain who receive only shoulder-focused treatment experience incomplete or temporary relief: the thoracic restriction driving the shoulder compensation remains unaddressed. Adding three to five minutes of thoracic mobility work to every upper body training session warm-up produces immediate improvements in overhead pressing mechanics that hours of shoulder-specific stretching alone cannot replicate. Research from NCBI on regional interdependence and shoulder function confirms that thoracic mobility interventions produce significant improvements in shoulder elevation range and reductions in impingement symptoms, even when the shoulder joint itself has adequate mobility.
Shoulder Mobility for Desk Workers: Addressing the Modern Epidemic
The combination of forward head position, rounded shoulders, and thoracic kyphosis that eight to ten hours of daily desk work produces has created a genuine epidemic of functional shoulder restriction in the working population. Adults who sit at computers for extended periods develop anterior chest tightness, thoracic kyphosis, and posterior capsule restriction as adaptive responses to the sustained seated forward-reach position that computing requires — the same restrictions that the shoulder mobility program in this article specifically addresses. The dose-response relationship between daily sitting hours and shoulder mobility restriction is well documented: each additional hour of daily sitting above six hours is associated with measurably reduced thoracic extension range and shoulder overhead mobility. The counterbalancing requirement — the amount of thoracic
Shoulder Mobility and Overhead Athletic Performance
Athletes in overhead sports — swimming, volleyball, baseball, tennis, gymnastics — require shoulder mobility that significantly exceeds the general population average, because their sports impose extreme ranges of motion under high-velocity loading that inadequate mobility cannot safely accommodate. Competitive swimmers require exceptional internal rotation during the pull phase and external rotation during recovery — ranges that require specific development beyond the general mobility work that most athletes perform. Volleyball attackers require the extreme external rotation range during the wind-up of attacking swings, with the same high-velocity deceleration demands as throwing athletes. Baseball pitchers require the most extreme shoulder external rotation of any athletic population — elite pitchers achieve 170-180 degrees of external rotation — and the inability to achieve this range forces compensatory loading patterns that produce the injuries that end pitching careers. For these athletic populations, the shoulder mobility program in this article provides the foundational work that prevents the restrictions that sport-specific training would otherwise create — performing the complete seven-exercise sequence daily maintains the mobility that these sports require while the sport-specific loading is applied in training and competition. The research on overhead sport injuries consistently identifies shoulder mobility restriction — particularly posterior capsule tightness and reduced external rotation — as a primary modifiable risk factor for injury in these populations, confirming that daily mobility maintenance is an investment in athletic longevity rather than an optional supplementary practice. According to research on shoulder mobility and overhead athlete injury, athletes with adequate external rotation range and posterior capsule flexibility show significantly lower injury rates than those with restriction in these specific mobility parameters.
When Shoulder Mobility Work Should Be Performed
The timing of shoulder mobility work within the training day affects both its effectiveness for flexibility development and its impact on subsequent training performance. Dynamic mobility work (wall slides, arm circles, band pull-aparts, thoracic rotation) performed before training sessions provides the activation and range preparation that improves pressing and pulling performance without the strength-reducing effects that static stretching produces. Static stretching (sleeper stretch, cross-body stretch, doorway pectoral stretch) performed immediately before heavy pressing can reduce strength output by five to eight percent — an unnecessary performance cost that justifies placing static work after training sessions rather than before them. The most evidence-based timing approach: dynamic shoulder preparation five minutes before training sessions (wall slides, band pull-aparts, arm circles), and static stretching after training sessions or as dedicated daily practice at a separate time (morning routine, evening routine, or post-training cool-down). This timing structure captures both the pre-training activation benefits of dynamic work and the flexibility development benefits of static work without the performance cost of pre-training static stretching. Daily consistent practice at a fixed time (regardless of training schedule) produces better flexibility outcomes than attempting to fit mobility work into training sessions that may be skipped or shortened by scheduling pressure. Research on static stretching and subsequent strength performance confirms that static stretching of thirty or more seconds duration performed immediately before strength training produces measurable reductions in subsequent strength output, validating the post-training or separate-session placement for static shoulder stretching.
Integrating Shoulder Mobility Into Your Existing Training Program
The seven-exercise shoulder mobility program integrates into any existing training schedule without requiring dedicated additional training sessions — the daily ten-minute practice fits into warm-up routines, cool-down periods, morning habits, or brief breaks throughout the workday. For athletes already training five to six days per week, the most practical integration: perform the dynamic components (wall slides, band pull-aparts, thoracic rotation) in the pre-training warm-up of every upper body session, and perform the static components (sleeper stretch, cross-body stretch, doorway stretch, foam roller) post-training or at a separate daily time. This distributes the complete program throughout the training week without requiring a dedicated shoulder mobility session. For athletes training three to four days per week, performing the complete ten-minute sequence before each training session provides sufficient daily frequency for meaningful mobility development while requiring no additional time commitment beyond the training schedule already in place. The key insight that makes the integration sustainable: shoulder mobility work before pressing sessions is not preparation time taken away from productive training but preparation that makes pressing training more productive and safer — a ten-minute investment that returns hours of better pressing quality across the weeks and months of training that follow. The integration therefore adds genuine value to every training session rather than merely adding time, which is the framing that makes daily shoulder mobility practice a welcomed rather than resented training component.
Programming Shoulder Mobility: Daily vs Session-Based Approaches
Shoulder mobility development responds to training frequency more than to session intensity — daily brief practice produces superior range of motion improvements compared to longer infrequent sessions. This frequency principle is particularly important for the connective tissue adaptations (posterior capsule lengthening, anterior chest flexibility) that require repeated low-intensity stimulus to remodel rather than the high-intensity loading that muscle hypertrophy requires.
The Daily 10-Minute Shoulder Mobility Protocol
Sleeper stretch: 3 × 30 seconds per side (3 minutes total). Cross-body stretch: 3 × 30 seconds per side (3 minutes total). Band pull-aparts: 3 × 15 repetitions (2 minutes total). Foam roller thoracic extension: 2 minutes at two positions. Total time: approximately 10 minutes. Performing this sequence daily — ideally before training sessions or as a morning routine — provides the continuous stimulus that drives capsule and tissue adaptation most efficiently. Research on flexibility development and training frequency consistently finds that daily stretching produces two to three times greater range of motion improvements than equivalent-volume less-frequent practice over eight-week study periods.
Pre-Training Shoulder Preparation
Before any upper body training session involving pressing or overhead work, a five-minute shoulder preparation sequence — foam roller thoracic extension (two minutes), wall slides (ten repetitions), band pull-aparts (fifteen repetitions), and arm circles (ten each direction) — prepares the shoulder for training loads by activating the posterior chain, improving thoracic extension, and establishing the shoulder position that allows safe pressing mechanics. This preparation is not a replacement for the daily mobility work but a training-specific warm-up that converts mobility gains into immediately usable range of motion for the session’s primary exercises. According to ACSM warm-up and injury prevention guidelines, sport-specific activation before upper body training significantly reduces shoulder injury risk and improves pressing performance quality.
Long-Term Shoulder Mobility Maintenance
Once functional shoulder mobility is achieved — the ability to perform the overhead reach test with both wrists touching the wall without lower back arching or elbow bending — the maintenance dose is significantly lower than the development dose. Five minutes of daily maintenance work (one set of sleeper stretch, one set of cross-body stretch, one set of band pull-aparts) preserves the mobility gains achieved through the initial development program. Discontinuing all shoulder mobility work after achieving good range typically results in gradual regression within four to eight weeks as the postural forces of daily life and pressing training reassert their tightening effects on the shoulder structures. Treating shoulder mobility maintenance as a permanent training component — five minutes daily, indefinitely — produces the lasting functional capacity that the initial investment in development was designed to create.
Action point: Schedule your daily 10-minute shoulder mobility practice at the same time each day this week — before morning coffee, immediately before training, or during a lunch break. The consistency of a fixed daily time produces dramatically better adherence than attempting to fit mobility work in whenever time allows.
extension and shoulder mobility work needed to offset each hour of sustained sitting — is approximately two minutes of targeted mobility work per hour of sitting. Office workers who sit eight hours per day therefore need approximately sixteen minutes of daily mobility work to maintain shoulder function, more than the standard ten-minute daily protocol this program prescribes for athletes whose sitting time is moderate. The practical solution: perform three to four minutes of thoracic extension (foam roller, chair back extension) and shoulder mobility during each work break, distributing the mobility work across the workday rather than attempting to reverse hours of postural adaptation in a single daily session. According to research on prolonged sitting and musculoskeletal health, distributed mobility breaks throughout the workday produce superior postural outcomes compared to equivalent total time of mobility work performed in a single session.
Shoulder Mobility Maintenance Across the Lifespan
Shoulder mobility naturally declines with age — research finds that overhead shoulder range decreases approximately five to ten degrees per decade after age 40 in sedentary adults, while adults who maintain deliberate shoulder mobility practice show dramatically slower decline. This age-related restriction primarily results from posterior capsule thickening, thoracic kyphosis progression, and rotator cuff changes that are not inevitable consequences of aging but adaptations to the reduced mobility demand of decreased physical activity. Adults who maintain upper body athletic activity — overhead pressing, swimming, tennis, climbing — throughout their fifties and sixties consistently show shoulder mobility profiles fifteen to twenty years younger than sedentary age peers, confirming that mobility maintenance through use is the most effective anti-aging intervention for shoulder function. The shoulder mobility program in this article, maintained as a permanent daily practice rather than a temporary rehabilitation protocol, provides the deliberate shoulder mobility stimulus that prevents the age-related decline that inactivity inevitably produces. Athletes who establish this daily practice in their thirties and maintain it through their sixties will have functional overhead capacity in their sixties that most sedentary adults lose in their forties — a genuinely meaningful quality-of-life difference that ten minutes of daily practice produces across decades of consistent application.
The Connection Between Shoulder Mobility and Neck Pain
Neck pain — one of the most prevalent musculoskeletal complaints affecting working adults — is frequently driven by the same postural restrictions that limit shoulder mobility, yet the connection between the two is rarely recognized in self-directed treatment. The forward head position that accompanies rounded shoulders places the cervical extensors in a chronically shortened, overworked state that produces the suboccipital tension headaches and neck stiffness that many desk workers accept as inevitable. Correcting the thoracic kyphosis and rounded shoulder posture that the shoulder mobility program addresses directly reduces the compensatory cervical forward position, allowing the neck musculature to return to the resting length that pain-free function requires. The lower trapezius strengthening from wall slides and band pull-aparts pulls the shoulders down and back, reducing the upper trapezius dominance that creates the neck and shoulder tension pattern that is so common in people who sit at computers for extended periods. Research on neck pain interventions consistently finds that thoracic and scapular mobility work produces greater neck pain reduction than neck-specific stretching and strengthening alone, confirming the regional interdependence relationship that makes the shoulder mobility program also a neck health program. Athletes who complete the shoulder mobility program daily for four to six weeks consistently report not only improved shoulder range but also reduced neck tension and headache frequency — the predictable consequence of addressing the postural drivers of neck dysfunction at their source rather than attempting to manage neck symptoms in isolation. According to research on regional interdependence in the cervicothoracic region, thoracic and scapular mobility interventions produce significant improvements in neck pain and cervical range of motion that cervical-specific interventions cannot equivalently achieve.
Shoulder Mobility for Swimmers: Specific Considerations
Swimmers develop shoulder mobility profiles that differ markedly from most gym athletes, with significant internal rotation and horizontal adduction from the pull phase and hypermobility in some directions alongside unexpected restrictions in others. The most common shoulder restriction in swimmers is not posterior capsule tightness (as in pressing athletes) but posterior shoulder weakness and scapular instability — the ability to achieve wide ranges of motion without the muscular control to stabilize the joint at those ranges. This instability pattern requires a different mobility program emphasis than the standard a
Common Questions About Starting the Shoulder Mobility Program
Before beginning the daily shoulder mobility program, most people have practical questions about how to fit it into their existing routine, what to expect in the first weeks, and how to know if it is working. When to perform the program: morning before coffee is the most consistently adhered-to timing because it requires no scheduling and creates a habitual morning anchor; alternatively, before any upper body training session captures the daily frequency needed while providing immediate performance benefit. What to expect in week one: mild discomfort in the posterior shoulder during the sleeper stretch (appropriate — this is the tight structure being loaded) and in the pectoral region during the doorway stretch (appropriate — anterior shortening being lengthened). Sharp pain anywhere (not appropriate — stop the exercise causing it). What improvement looks like by week two: the sleeper stretch should feel slightly less intense, and the overhead wall reach should achieve slightly greater range than week one. Quantifying this improvement requires measurement — use a measuring tape to record how far the wrists are from the wall in the overhead reach test at weeks one, two, four, and eight. The objective measurements reveal improvement that subjective perception often misses during the gradual daily practice. Is it working after two weeks without obvious improvement: continue. Connective tissue adapts more slowly than muscle — four to six weeks is the typical timeline for meaningful capsule and fascial length changes to become measurable. The daily practice is working during this period even when it does not yet feel like it; the structural changes are occurring at the cellular level before they express as measurable range improvement. JOSPT clinical guidelines on shoulder mobility programs recommend four to six week minimum trial periods before assessing program effectiveness for capsular and fascial restrictions.
When Shoulder Pain Requires Professional Evaluation
The shoulder mobility program described in this article is appropriate for functional mobility restriction — the stiffness and limited range that results from postural habits, training imbalances, and sedentary lifestyle. Several shoulder presentations require professional medical evaluation before beginning any mobility or strengthening program, because these presentations may indicate structural pathology that the self-directed program is not appropriate to address.
Presentations Requiring Medical Evaluation
Sharp or electric pain during any shoulder movement (rather than the dull stretch sensation of mobility work) suggests nerve involvement or structural damage that warrants imaging and professional assessment. Pain that worsens consistently during or after mobility exercises rather than improving over two to four weeks of consistent practice indicates that the exercises may be aggravating rather than addressing the source of restriction. Night pain — shoulder pain that wakes from sleep or prevents comfortable sleep positions — is a red flag for rotator cuff pathology that requires ultrasound or MRI assessment. Any shoulder pain following trauma (fall, collision, or sudden force) should be evaluated for fracture, dislocation, or ligamentous damage before returning to training. Significant asymmetry in passive range of motion (one shoulder dramatically more restricted than the other without prior injury explaining the difference) warrants professional assessment to rule out adhesive capsulitis (frozen shoulder), which responds poorly to self-directed mobility work and requires specific clinical treatment.
Working With Healthcare Providers
Sports medicine physicians, physical therapists specializing in shoulder conditions, and certified strength and conditioning specialists with shoulder expertise can provide individualized assessment that identifies whether mobility restriction, strength imbalance, or structural pathology is the primary limiting factor. Physical therapists can prescribe specific manual therapy techniques (joint mobilization, soft tissue treatment) that accelerate improvement beyond what self-directed mobility work alone can produce, particularly for significant posterior capsule restriction and adhesive capsulitis. When self-directed mobility work produces no measurable improvement after six to eight weeks of consistent daily practice, professional evaluation is the appropriate next step rather than simply continuing the same intervention for longer. According to NSCA guidelines for exercise and shoulder health, professional evaluation is recommended when shoulder mobility restriction persists despite appropriate self-directed intervention or when training-related shoulder pain does not resolve with load reduction and targeted mobility work.
Action point: If you have had shoulder pain or discomfort for more than six weeks that has not improved with rest, consult a sports medicine physician or physical therapist before beginning this mobility program. Most functional shoulder restriction resolves with the program described — but getting professional confirmation that the restriction is functional rather than structural prevents the risk of aggravating genuine pathology with inappropriate exercise.
The Rotator Cuff: Understanding the Muscles That Protect Your Shoulder
The rotator cuff — four muscles (supraspinatus, infraspinatus, teres minor, subscapularis) that surround the glenohumeral joint — is both the shoulder’s primary dynamic stabilizer and the structure most commonly injured in overhead and pressing activities. Understanding each muscle’s function guides targeted strengthening that prevents the rotator cuff weakness that causes impingement and tears. The supraspinatus initiates the first fifteen degrees of shoulder abduction and contributes to the humeral head depression that prevents impingement during overhead elevation — it is the most commonly torn rotator cuff muscle and the most important for overhead function. The infraspinatus and teres minor externally rotate the humerus and decelerate the arm after overhead throwing — crucial for overhead sport athletes and significantly undertrained in pressing-dominant programs. The subscapularis internally rotates the humerus and contributes to anterior stability — typically adequately developed through pressing, but requiring balanced training alongside the external rotators to prevent the internal rotation dominance that causes impingement. The face pull and band pull-apart exercises in this program specifically target the infraspinatus and teres minor — the external rotators that are most chronically undertrained relative to the internal rotators developed by pressing. Consistent external rotation strengthening through these exercises maintains the rotator cuff balance that protects the supraspinatus from the impingement forces that internal rotation dominance creates. According to research on rotator cuff muscle imbalances, athletes who perform regular external rotation strengthening show significantly lower rates of rotator cuff pathology than those who train with pressing emphasis without balancing external rotation work.
Shoulder Mobility and Sleep Position
Sleep position contributes significantly to shoulder mobility restriction and shoulder pain in ways that most people never consider — spending six to eight hours in a position that compresses one shoulder against the mattress or maintains the arm in an internally rotated position creates the same postural adaptation that hours of desk work produces. Side sleepers who consistently sleep on one side often develop greater posterior capsule tightness on the weight-bearing shoulder, explaining the asymmetric shoulder mobility restrictions that many athletes experience despite symmetric training. The most shoulder-fpproach described in this article: less capsule stretching (which further increases range in already hypermobile joints) and more strengthening at end ranges (external rotation strengthening in the externally rotated position, scapular stabilizer strengthening at fully elevated arm positions). For non-swimming gym athletes, the program as described is appropriate. For competitive swimmers who perform the program alongside heavy swim training, reducing the sleeper stretch and pectoral stretch components (which may increase instability in already mobile swimmer shoulders) and emphasizing band pull-aparts and external rotation strengthening provides the shoulder health stimulus appropriate for this specific population. Consulting a sports physical therapist who specializes in swimming shoulder injuries provides individualized guidance that the general program cannot offer for athletes with complex overhead sport demands.
The Shoulder Mobility Program for Strength Athletes
Powerlifters, Olympic weightlifters, and CrossFit athletes have specific shoulder mobility needs determined by their competitive demands. Olympic weightlifters require extreme overhead mobility for the catch positions of the snatch and clean and jerk — the overhead squat position’s shoulder demands exceed what the standard program addresses, and weightlifters benefit from additional overhead flexibility work including overhead squat holds, snatch-grip overhead squats, and wrist mobility specific to the snatch grip. Powerlifters primarily need posterior capsule flexibility (for bench press shoulder health) and thoracic extension (for overhead positioning in competition) — the sleeper stretch and foam roller thoracic extension are the most relevant components of the standard program for this population, while overhead-specific components are less relevant. CrossFit athletes need the complete mobility profile — overhead for pressing and gymnastics, posterior capsule for bench and ring work, thoracic extension for kipping and overhead stability — making the complete seven-exercise program most appropriate for this multi-modal athletic population. The shoulder mobility program’s strength is its comprehensiveness; individual athletes with specific sport demands may appropriately modify the emphasis to match their primary mobility requirements while maintaining the daily practice frequency that produces results regardless of the specific exercises emphasized. According to NSCA sport-specific conditioning guidelines, flexibility programming for strength athletes should be matched to the specific mobility demands of the primary competitive movements rather than applied generically across all athletes regardless of sport demands.
Shoulder Mobility and Strength Training for Youth Athletes
Young athletes (ages twelve to eighteen) who begin strength training before their shoulder mobility patterns are established have the opportunity to develop excellent shoulder function from the beginning rather than correcting the restrictions that adult training often creates. Youth athletes who learn proper shoulder mechanics — upright posture, scapular retraction during pulling, external rotation maintenance during pressing — from the beginning of their training experience avoid the years of postural adaptation that create the restrictions the adult shoulder mobility program is designed to reverse. For youth athletes already training, incorporating the band pull-apart and wall slide exercises as standard components of every upper body warm-up takes five minutes and develops the posterior shoulder chain balance that protects against the shoulder injuries that overhead sport participation increasingly produces in young athletes. Research on shoulder injury prevention in youth overhead athletes consistently identifies early strength training for the rotator cuff and scapular stabilizers as the intervention with the greatest injury risk reduction — making the preventive application of this program for young athletes even more valuable than its rehabilitative application for adults with established restrictions. Youth coaches and parents who introduce shoulder mobility and posterior chain strengthening early in athletic development contribute to the long-term shoulder health that allows decades of athletic participation without the injuries that neglected shoulder balance produces. According to research on shoulder injury prevention in youth athletes, early strengthening programs for the posterior shoulder significantly reduce injury rates in youth populations engaged in overhead sports.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Consistent practice across weeks and months reveals the compound returns that any single training session cannot demonstrate. The exercises described in this article work — the research supporting them is clear, the practical evidence from athletes who use them consistently is compelling, and the physiological mechanisms that produce their results are well understood. What they require from the athlete is the patience to apply them consistently across the training timelines that meaningful physical development demands. Apply them with that patience and discover the results that the research and experience of thousands of athletes before you confirm are waiting on the other side of consistent effort.
Frequently Asked Questions About Shoulder Mobility
How long does it take to improve shoulder mobility significantly?
Most people with moderate shoulder mobility restriction notice meaningful improvement within two to four weeks of daily mobility practice — the overhead reach test typically improves by ten to twenty degrees within this timeframe. Reaching full functional overhead mobility from a significantly restricted baseline (unable to reach the wall overhead without compensations) typically requires eight to twelve weeks of consistent daily practice. Adhesive capsulitis (frozen shoulder) requires significantly longer — typically six to twelve months of dedicated treatment — and generally requires professional intervention rather than self-directed mobility work alone. The most important factor in improvement rate is practice frequency: daily practice produces two to three times faster improvement than twice-weekly practice at equivalent total time, because connective tissue remodeling requires repeated daily stimulus rather than the infrequent higher-intensity work that drives muscle hypertrophy. According to research on flexibility training frequency, daily stretching programs produce significantly faster range of motion improvements than equivalent-volume lower-frequency programs.
Can I train upper body while improving shoulder mobility?
Yes — training and mobility development can occur simultaneously, and in many cases the training sessions provide valuable feedback about which mobility restrictions most limit performance. Modify training as needed to accommodate current range: use dumbbells instead of a barbell for pressing if the bar path creates shoulder pain (dumbbells allow the arms to travel in the path that each shoulder’s current range allows rather than the fixed path the barbell requires); reduce overhead pressing load until mobility improves; and avoid movements that consistently reproduce sharp pain regardless of load. The mobility work should be performed before training sessions (as a warm-up) and daily on non-training days to maximize improvement rate while allowing continued training in the movements that current range permits.
Are shoulder mobility restrictions permanent?
Functional shoulder mobility restrictions — those caused by capsule tightness, muscular imbalance, and postural habits rather than structural pathology — are not permanent and respond predictably to targeted mobility work and postural correction. Even long-standing restrictions (present for years) typically show measurable improvement within four to six weeks of consistent targeted intervention. Structural limitations from significant rotator cuff tears, significant labral damage, or significant bony abnormalities may limit the maximum achievable range — but the functional restriction that most recreational athletes experience is not structural and responds well to the approaches described in this article. The most important insight: shoulder mobility restriction that developed over months and years of poor posture and training imbalance requires months of consistent correction to fully resolve — but that resolution is achievable for virtually all healthy adults who apply the program consistently.
Should I stretch before or after training?
Static stretching (the held-position stretches like sleeper stretch and cross-body stretch) performed immediately before training can temporarily reduce strength output by five to eight percent — this is the basis for recommendations to avoid static stretching before strength training. Dynamic mobility work (wall slides, arm circles, band pull-aparts) does not produce this performance reduction and is appropriate before training. The practical approach: perform dynamic shoulder preparation (wall slides, band pull-aparts, arm circles) before training sessions and perform static stretching after training sessions or as a separate daily practice outside training time. This captures both the pre-training activation benefits of dynamic work and the flexibility development benefits of static stretching without the performance cost of pre-training static stretching.
riendly sleep position is on the back with the arms at the sides — this eliminates shoulder compression and maintains the shoulder in a neutral position throughout the sleep period. For dedicated side sleepers, sleeping with a pillow between the arm and the body (preventing the shoulder from compressing) and avoiding the “praying mantis” position (arm bent at the shoulder across the chest) minimizes the shoulder compression that contributes to mobility restriction. Athletes with significant shoulder pain that is worse in the morning than the evening should specifically evaluate their sleep position as a potential contributor to the overnight muscle guarding and positional stress that morning pain reflects. Addressing sleep position alongside the daily mobility program described in this article produces faster resolution of shoulder restrictions that sleep-related compression perpetuates.
Shoulder Mobility and Breathing: The Unexpected Connection
Breathing mechanics — specifically the pattern of thoracic expansion during inhalation — directly affects shoulder mobility through the shared mechanical relationship between the rib cage, thoracic spine, and shoulder girdle. Shallow upper chest breathing (common in people with chronic stress and poor posture) relies on the secondary breathing muscles — scalenes, sternocleidomastoid, and upper trapezius — rather than the diaphragm, creating chronic tension in the neck and upper shoulder region that contributes to the shoulder elevation and forward head position that limits overhead mobility. Diaphragmatic breathing (belly breathing that expands the lower rib cage rather than raising the chest) reduces this secondary muscle recruitment, allowing the neck and upper shoulder muscles to relax and improving the cervicothoracic mobility that overhead shoulder function requires. Incorporating three to five minutes of deliberate diaphragmatic breathing practice before the shoulder mobility program activates the parasympathetic nervous system, reduces upper trapezius tension, and prepares the thoracic spine for the extension work that follows. This breathing-mobility integration is standard practice in yoga and Pilates traditions and is increasingly supported by research on the relationship between breathing patterns and musculoskeletal function. According to research on breathing patterns and musculoskeletal function, diaphragmatic breathing training significantly reduces secondary muscle hypertonicity in the neck and shoulder region, improving thoracic mobility and overhead function as a secondary effect.
Tracking shoulder mobility progress requires consistent measurement methodology to distinguish genuine range improvements from day-to-day variation that temperature, sleep quality, and recent activity produce. The most reproducible assessment approach: perform all three assessments at the same time of day (ideally morning before warming up or exercise), after at least six hours of sleep, and after the same brief standardized preparation (five arm circles in each direction). Under these standardized conditions, measurements taken monthly reveal the genuine mobility progression that the daily practice is producing rather than the apparent variation that inconsistent testing conditions create. Photographing the overhead reach test and the behind-back reach test monthly against a consistent background creates a visual record of progress that motivates continued practice more powerfully than abstract range measurements. Many athletes who begin the program unable to touch the wall overhead with both wrists (without lower back arching) reach this milestone within six to eight weeks of daily practice — a transformation that photographs document clearly and that before-and-after comparison makes immediately compelling evidence of the program’s effectiveness. The documented evidence of real range improvement is the most powerful motivator for maintaining the daily mobility practice that continuing improvement requires. Athletes who see their overhead reach improve by five to ten centimeters on monthly photographs are dramatically more likely to maintain the daily practice that produced it than those who track only subjectively and fail to register the gradual improvements that objective measurement reveals. NSCA assessment guidelines support standardized, periodic fitness assessment as a primary tool for maintaining training motivation and optimizing program adjustments across long-term development periods.
The Shoulder Mobility Program as Preventive Healthcare
Investing ten minutes daily in shoulder mobility work before shoulder pain develops is dramatically more efficient than the weeks of physical therapy, exercise modification, and performance reduction that recovering from shoulder impingement or rotator cuff issues requires. The ten-minute daily investment prevents problems that would require months to resolve and potentially involve imaging, professional treatment, and training interruption that together cost far more time and money than daily prevention requires. This preventive framing — treating shoulder mobility maintenance as healthcare rather than optional training enhancement — is consistent with how evidence-based medicine approaches musculoskeletal health: the best intervention is prevention applied before pathology develops, not treatment applied after it does. Adults in their thirties who establish daily shoulder mobility practice prevent the functional restrictions that sedentary adults commonly experience in their forties and fifties, maintaining the shoulder function that daily activities, recreational sports, and strength training require for active living across decades. The shoulder, as the most mobile and consequently most injury-prone major joint, rewards this preventive investment more than almost any other joint — its complexity means that problems once established are difficult to fully resolve, making the daily investment in preventing those problems a genuinely high-value healthcare activity for any physically active adult. ACSM preventive exercise guidelines identify regular flexibility and mobility maintenance as evidence-based preventive practices that reduce musculoskeletal injury risk across all active adult populations.
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. The Fitness Quality Nobody Trains Until It Fails Them Balance is…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Medical Disclaimer: This article is for general informational purposes only and does not constitute medical advice. If you are…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Medical Disclaimer: This article is for general informational purposes only. If you are experiencing joint pain or any health…
Warning Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. Warning Medical Disclaimer: This article is for general informational purposes only…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Medical Disclaimer: This article is for general informational purposes only. If you are experiencing pain or any health condition,…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Exercise carries inherent risks. Always consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program, especially if you have a pre-existing medical condition, injury, or health…