⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program.
⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain medical clearance from your physician before performing high-intensity training.
The Cardio Plateau That Feels Like Hard Work But Produces Nothing
I spent eighteen months doing cardio three times a week, every week, without missing a session. My weight never changed. My resting heart rate never dropped. My endurance improved slightly in the first two months and then flatlined. I was consistent, I was sweating, I was checking every box — and the boxes were wrong.
When I finally had a proper fitness assessment, the results were humbling. My cardiovascular fitness was modestly above average for a sedentary adult despite eighteen months of regular training. The tester asked me what I was doing for cardio. I described my sessions: thirty to forty minutes at a pace that felt comfortably hard, three times a week. She nodded. “You’re training in the adaptation zone for beginners consistently,” she said. “Your body adapted to exactly this stimulus in the first two months and has had no reason to change since.”
Cardio that isn’t working isn’t usually a consistency problem — it’s a stimulus problem. The five mistakes in this article explain why your cardiovascular training is producing effort without adaptation, and each comes with a specific, actionable fix that begins working within weeks.
Why the Body Stops Responding to Cardio
The human body adapts to training stimuli with remarkable efficiency — and then stops adapting when the stimulus no longer exceeds its current capacity. Cardiovascular adaptation requires that training intensity, duration, or frequency exceeds what the system has already adapted to handle. The same thirty-minute jog at the same pace that challenged you six months ago provides essentially no cardiovascular development stimulus today because your heart, lungs, and trained muscles can handle it without strain. This accommodation is not failure — it is success at adaptation that requires a new challenge to continue producing results.
The Cardio Paradox: Working Hard But Getting Nowhere
The frustrating experience of training consistently, sweating through sessions that feel genuinely hard, and seeing no measurable improvement in cardiovascular fitness is far more common than fitness culture acknowledges. Most people blame effort when the real problem is approach — they are working hard in ways that do not produce the specific physiological stimulus that cardiovascular improvement requires. The five mistakes that kill cardio results share a common thread: they produce subjective effort without the targeted physiological stimulus that drives measurable adaptation. Understanding the difference between effort that feels productive and effort that is biologically productive is the insight that transforms stagnant cardio from frustrated repetition into meaningful progress. ACSM cardiovascular training guidelines identify training specificity, progressive overload, and appropriate intensity distribution as the primary determinants of cardiovascular adaptation — the same factors that the five mistakes described in this article systematically undermine.
The Adaptation Plateau: What It Is and Why It Happens
The body’s adaptive response to cardiovascular training is fundamentally conservative — it adapts precisely to the demands imposed, then stops adapting once those demands are met. This conservation is physiologically sensible: adaptation requires energy, and the body does not invest in adaptation beyond what the environment demands. For the recreational athlete, this means that every cardio routine eventually stops producing results — not because the routine is bad, but because the body has adapted to it and no longer needs to change to meet its demands. The timeline varies: beginners see adaptation for six to twelve weeks on any consistent program; intermediates plateau within four to six weeks on an unchanged program; advanced athletes may plateau within two to three weeks on programs that do not systematically vary stimulus. Recognizing the adaptation plateau as a normal biological phenomenon rather than personal failure reframes the appropriate response — not more of the same effort, but systematic stimulus variation that provides the novel demand that drives continued adaptation. The five mistakes in this article represent the five most common ways athletes fail to provide the novel stimulus that continued improvement requires.
The Specificity of Cardio Adaptation: Training for What You Want
Cardiovascular adaptation is highly specific to the demands of the training stimulus — a principle called training specificity that explains why different cardio approaches produce different outcomes. Running-specific adaptations improve running performance but transfer only partially to cycling; high-intensity interval adaptations improve VO2 max but do not develop the fat oxidation machinery that Zone 2 training builds; steady-state adaptations develop aerobic base but do not develop the lactate threshold capacity that interval training builds. This specificity means that training for the wrong goal — doing high-intensity intervals when aerobic base is the limiting factor, or doing Zone 2 exclusively when lactate threshold development is needed — produces effort without the specific outcome targeted. Diagnosing which adaptation is currently limiting performance and targeting training specifically at that adaptation produces faster improvement than general cardiovascular effort without diagnostic direction. The five mistakes in this article represent the five most common specificity failures — training that expends effort without targeting the specific physiological stimulus that would produce the desired improvement. Correcting them requires not more effort but more specific effort directed at the actual limiting adaptation.
Every athlete who has broken through a cardio plateau using the approaches described in this article reports the same experience: a period of uncomfortable change followed by measurable improvement that validates the discomfort. The discomfort of Zone 2 training that feels too easy, Zone 4 training that feels genuinely hard, and systematic progression that requires planning rather than habit — these are the specific discomforts that produce the cardiovascular improvements that comfortable, familiar gray-zone training cannot generate. Embrace the discomfort of the correct approach and the results follow reliably.
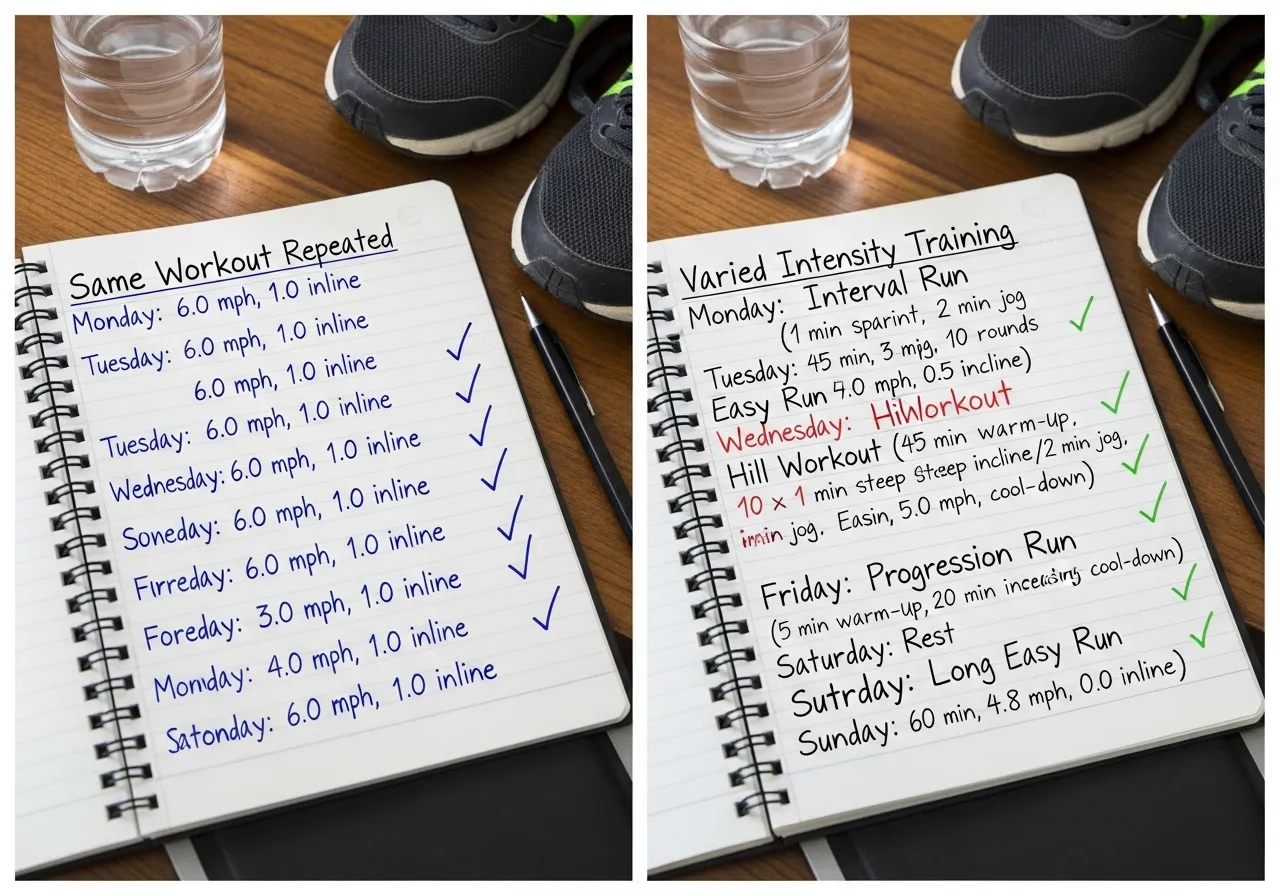
Mistake 1: You Have Been Doing the Same Workout for Too Long
Identical training — same duration, same intensity, same exercise, same frequency — produces identical adaptation until the body fully adapts, and then it produces nothing. Most people who report that cardio “stopped working” have been doing essentially the same sessions for three to six months without any meaningful variation. This is not a metabolism problem, a hormonal problem, or a genetic ceiling — it is an accommodation problem with a straightforward solution: change the stimulus.
The Three Variables to Change
Intensity: if you have been training at a consistent moderate pace, introduce either Zone 2 base sessions (slower than your current pace, focused on aerobic development) or Zone 4 to 5 interval sessions (harder than your current pace, focused on VO2max development). The introduction of either extreme relative to your current middle-intensity training is almost guaranteed to produce new adaptations. Duration: extend one session per week by 15 to 20 minutes beyond your normal length. Longer sessions at aerobic intensity develop cardiovascular endurance adaptations that shorter sessions at the same intensity cannot produce. Modality: switching from running to cycling, rowing, or swimming forces cardiovascular adaptation through different muscular patterns and challenges the cardiovascular system in ways it has not fully adapted to from your primary modality.
How Long Before Accommodation Occurs
Most intermediate cardiovascular adaptations occur within six to eight weeks of a new stimulus. After this period, the same stimulus produces maintenance rather than improvement. A practical guideline: if your performance at a given effort level — heart rate at a fixed pace, pace at a fixed heart rate — has not improved in six weeks, your training stimulus has been fully accommodated and requires modification. Measuring this performance metric every four to six weeks provides the data to make evidence-based decisions about when to change training variables. ACSM cardiorespiratory fitness guidelines recommend progressive increase in training demands as the foundation of continued cardiovascular improvement at all fitness levels.
Action Point
Write down the exact details of your last five cardio sessions — duration, intensity, modality. If they are essentially identical, introduce one of the three variables listed above in your next session. Track whether the new stimulus feels different from your previous training. If it does, adaptation is occurring. If it feels exactly the same as your old training, the change was insufficient.
Mistake 1 Deep Dive: The Three Types of Variation That Break Accommodation
Workout accommodation — the body’s complete adaptation to a specific training stimulus — makes the identical workout progressively less effective over time. The three types of variation that specifically prevent accommodation are intensity variation (changing the heart rate zone distribution), volume variation (changing total weekly cardiovascular duration), and modality variation (changing the exercise type). Intensity variation is most important: if you always run at the same pace for the same duration, the cardiovascular system adapts precisely to that demand and stops improving. Adding one higher-intensity interval session and one longer lower-intensity session per week while maintaining the remaining sessions at standard intensity provides sufficient variation to prevent accommodation in most intermediate athletes. Volume variation — progressively increasing weekly duration over four to six weeks before reducing for a recovery week — follows the same periodization principle that produces continued strength gains in resistance training. Modality variation — alternating between running, cycling, swimming, and rowing across training weeks — develops the cardiovascular system from multiple biomechanical angles and prevents the overuse patterns that single-modality training at high volumes produces. Implementing all three types of variation simultaneously produces the most comprehensive accommodation prevention; implementing even one prevents the complete stagnation that characterizes true accommodation plateau.
The Minimum Effective Dose of Variation
For athletes concerned that adding variation will disrupt a routine that was working until the plateau, the minimum effective dose of variation is worth knowing. Research on training accommodation and variation suggests that changing one training variable every four to six weeks is sufficient to prevent full accommodation plateau while maintaining enough consistency for adaptation to compound. In practical terms: run the same four sessions per week but change the intensity distribution of one session (from steady moderate to interval training) every four to six weeks; or maintain the same weekly structure but progressively increase session duration by five minutes every two weeks. These small, systematic changes provide the novel stimulus that prevents accommodation without the disruption of completely overhauling a training program. The athlete who makes these small systematic adjustments continues progressing indefinitely, while the one who maintains identical training stagnates within months. Research on training variation and cardiovascular adaptation confirms that systematic variation of at least one training variable prevents accommodation plateau and maintains progressive cardiovascular adaptation across extended training periods.
The most important insight about cardio mistakes is that they are not failures of effort but failures of approach — hard work directed at the wrong stimulus produces hard work’s exhaustion without the specific physiological adaptations that produce improvement. Redirecting identical effort toward the correct stimulus produces the results that the same effort previously failed to generate. The cardio athlete who makes this shift consistently reports feeling like training suddenly became productive after months of stagnation — not because effort increased, but because the same effort finally became biologically specific to the adaptations that drive measurable improvement.
Mistake 2: You Are Training in the Gray Zone Where Nothing Happens
The cardiovascular gray zone is the moderate intensity range — roughly 70 to 80 percent of maximum heart rate — that is simultaneously too hard to produce the deep aerobic adaptations of true low-intensity Zone 2 training and too easy to produce the VO2max and performance adaptations of genuine high-intensity training. It is the zone of effort without proportionate reward, and it is where most recreational athletes spend most of their training time.
Why the Gray Zone Is So Common
The gray zone is comfortable in a way that feels productive. It’s hard enough to feel like real exercise, hard enough to generate sweat and fatigue, but not so hard that it requires genuine discipline to sustain. Zone 2 training feels embarrassingly slow — people worry others in the gym will judge their pace. Zone 5 training requires genuine discomfort that many avoid. The gray zone is what happens in the absence of structure: not deliberately chosen but naturally arrived at by people who want to feel like they’re working without genuinely challenging themselves.
The Fix: Polarized Training
Research on training intensity distribution consistently shows that elite endurance athletes perform approximately 80 percent of their training at low intensity (Zone 1 to 2) and 20 percent at high intensity (Zone 4 to 5), with minimal time in the moderate gray zone. Research on polarized training distribution in endurance athletes finds this polarized approach produces superior cardiovascular development compared to moderate-intensity dominant training at equivalent volumes. For recreational athletes, implementation: consciously slow down your easy sessions until they’re genuinely Zone 2 (full-sentence conversation possible throughout), and add one weekly session where you genuinely push into Zone 4 to 5 intensity. Eliminate the middle.
Action Point
On your next cardio session, apply the talk test throughout. If you cannot speak full sentences, slow down until you can. Maintain this genuinely easy pace for the entire session. Then add one session this week where you perform 6 times 1-minute hard efforts with 1-minute easy recovery between each. Two weeks of this polarized structure will feel dramatically different from gray zone training — and will produce visible fitness improvement within four weeks.
The Gray Zone Problem: Why Moderate Intensity Produces Minimal Results
The gray zone — cardiovascular training at 65-80% of maximum heart rate, where effort feels significant but conversation is possible with effort — is simultaneously the most popular and least effective intensity range for cardiovascular development. Its popularity is psychological: it feels hard enough to feel productive but not so hard that it requires genuine discomfort. Its ineffectiveness is physiological: it is too intense to drive the mitochondrial biogenesis and fat oxidation adaptations of Zone 2, yet not intense enough to drive the lactate threshold development and VO2 max improvements of Zone 4-5. The gray zone produces the metabolic cost of moderate effort without the specific adaptations of either lower or higher intensity training — a physiological no-man’s land that creates an illusion of productivity through sweat and effort while providing minimal cardiovascular stimulus for the time invested.
The polarized training approach — spending 80% of cardiovascular volume in Zone 2 and 20% in Zone 4-5, with minimal time in Zone 3 — is supported by research on elite endurance athletes and is increasingly validated in recreational athlete populations. Elite endurance coaches across running, cycling, and rowing have converged on this distribution independently because their athletes’ performance data supports it. Recreational athletes who shift from gray-zone-dominated training to polarized distribution typically see improved performance within six to eight weeks, because they are finally providing the specific stimuli that drive Zone 2 aerobic base development and Zone 4-5 performance ceiling improvement simultaneously. The transition requires discipline — Zone 2 training feels embarrassingly easy, and Zone 4-5 training requires genuine discomfort — but the results validate the discomfort of abandoning the psychologically comfortable gray zone. Research on polarized training distribution consistently demonstrates superior performance outcomes compared to moderate-intensity dominated training in both recreational and competitive endurance athletes.
Concurrent Training: Managing Cardio and Strength Without Interference
The interference effect — where excessive cardio volume impairs strength and muscle development — is a real but manageable concern for athletes who combine cardiovascular and resistance training. Managing it effectively requires understanding which types of cardio create the most interference (high-intensity, high-volume endurance work) and which create minimal interference (low-to-moderate intensity Zone 2 work of moderate duration). Zone 2 cardiovascular training at two to three sessions per week of thirty to sixty minutes produces essentially no interference with strength and muscle development in research on concurrent training, because its low intensity does not produce the sustained high-cortisol environment that high-intensity endurance training creates. Scheduling cardio sessions on separate days from strength sessions, or at least six hours apart when same-day training is necessary, further minimizes interference by allowing recovery between the two training stimuli. The practical concurrent training approach that minimizes interference: two to three Zone 2 cardio sessions per week on non-lifting days or at separate times from lifting, plus one HIIT session per week (scheduled away from lower body lifting days). This combination develops cardiovascular fitness alongside strength without the interference that higher-volume or higher-intensity cardio imposes. Research on concurrent training interference confirms that moderate Zone 2 volume produces minimal interference with strength development when appropriately scheduled, while high-intensity endurance training at high volumes produces significant interference that requires careful management.
Most recreational athletes spend the majority of their cardio time in Zone 3 not because they intend to but because Zone 2 feels insufficiently challenging and Zone 4-5 requires genuine discomfort — Zone 3 is the path of least resistance that heart rate monitoring consistently reveals as the dominant training zone for athletes who train by feel. Correcting this with objective zone monitoring produces the cardiovascular development that gray-zone training systematically fails to generate despite the genuine effort it requires.
Mistake 3: Your Weekly Volume Is Insufficient for the Goals You Have
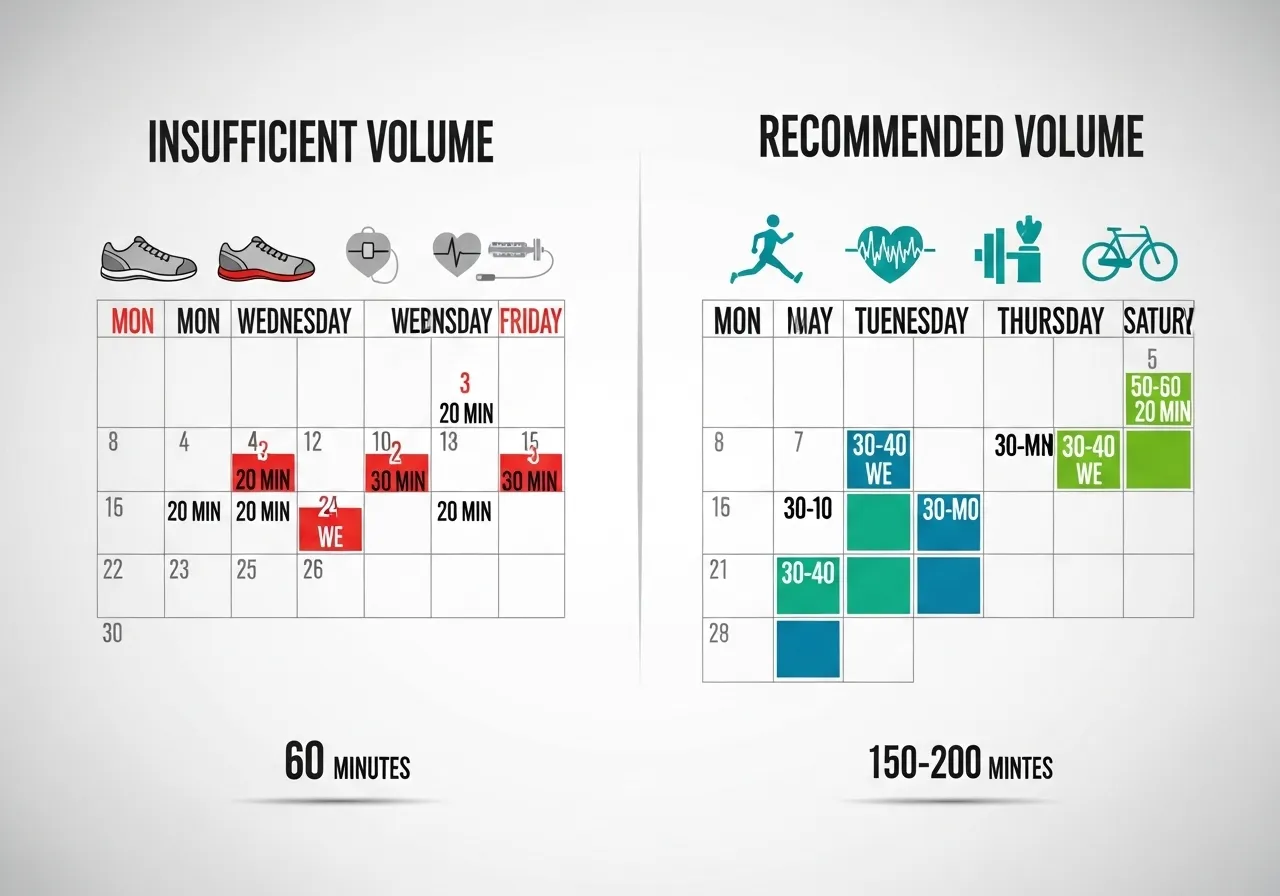
A fundamental mismatch between training volume and desired outcomes is one of the most common reasons cardio stops producing results — or never started producing the results people expected. The research on exercise and health outcomes is clear: the relationship between cardiovascular exercise volume and benefit is dose-dependent, with more volume producing more benefit up to a high ceiling. Three thirty-minute sessions per week produces health improvement. It produces much less weight management effect or performance improvement than the same three hours distributed differently or extended to four to five sessions.
Volume Requirements by Goal
General cardiovascular health: 150 minutes per week of moderate intensity or 75 minutes per week of vigorous intensity — the WHO and ACSM minimum recommendation. This volume reduces cardiovascular disease risk significantly but produces modest fitness and minimal body composition change. Fat loss support: 200 to 300 minutes per week of moderate intensity, producing 1,000 to 2,000 calories per week of additional caloric expenditure that can support a meaningful caloric deficit. Performance improvement: 300 to 450 minutes per week for recreational athletes pursuing fitness as a serious goal — the volume at which meaningful cardiovascular performance development consistently occurs. If your current volume is 90 minutes per week and you expect significant fat loss or fitness improvement, the mismatch between volume and expectation is the primary problem.
Building Volume Safely
The 10 percent rule: increase total weekly cardiovascular volume by no more than 10 percent per week to reduce overuse injury risk. Adding volume too rapidly — particularly in running and jumping activities — produces the musculoskeletal overuse injuries that are the most common cause of cardio program abandonment. Extend session duration before adding sessions: an extra 10 minutes per session across three sessions adds 30 minutes to weekly volume without the schedule disruption of adding a fourth training day.
Action Point
Calculate your current weekly cardiovascular training volume in minutes. Compare it to the volume range appropriate for your goals from the list above. If there is a significant gap, build toward the target volume at the 10 percent per week rate over the coming weeks. The volume gap between current training and goal-appropriate training may explain more of your results plateau than any other single factor.
Building Weekly Cardio Volume That Actually Produces Results
Insufficient weekly cardiovascular volume is a significant and commonly overlooked cause of cardio plateaus — many recreational athletes train at adequate intensity but for too few total minutes per week to drive continued adaptation. Research on cardiovascular training volume and adaptation finds that meaningful aerobic base development requires a minimum of 150-200 minutes of Zone 2 training per week, with greater volumes producing proportionally greater adaptations up to approximately 400-500 minutes per week for recreational athletes. Below 150 minutes per week, Zone 2 training primarily maintains current fitness rather than developing it further. Many recreational athletes who train three sessions of 30-40 minutes per week are getting 90-120 minutes of total cardiovascular volume — enough for health maintenance but insufficient for meaningful fitness improvement beyond their initial adaptation phase. Building to 200+ minutes per week of Zone 2 training, even at the cost of reducing session intensity to maintain zone compliance, consistently produces the cardiovascular improvements that lower-volume training stagnated on.
The Progression Plan: Adding Volume Without Getting Injured
Adding cardiovascular volume too quickly produces the overuse injuries that interrupt training and erase accumulated adaptation. The 10% weekly volume increase rule — never increasing total weekly cardiovascular duration by more than 10% in a single week — provides a conservative progression rate that most cardiovascular systems can accommodate without overuse injury. Starting from 120 minutes per week and applying the 10% rule reaches 200 minutes within seven weeks and 300 minutes within fourteen weeks — a practical timeline for building the volume that drives meaningful cardiovascular development. Every four to six weeks of volume building should be followed by a recovery week of 60-70% normal volume, allowing accumulated tissue stress to resolve before the next building phase. This structured approach — build, recover, build higher — produces continuous cardiovascular improvement across months without the training interruptions that aggressive volume increases produce. The patience required by this approach is the same patience that produces the long-term cardiovascular development that short-term high-intensity-only approaches cannot match. Research on training load progression and injury prevention supports conservative volume increases as the primary modifiable factor in preventing cardiovascular training overuse injuries across all populations and experience levels.
Cardio Periodization: Planning for Long-Term Cardiovascular Development
Applying periodization principles to cardiovascular training — systematically varying volume and intensity across planned multi-week cycles — produces superior long-term development compared to maintaining the same training approach year-round. A simple four-phase cardio periodization cycle: base phase (eight to twelve weeks), emphasizing Zone 2 volume building at 80%+ of total cardio in Zone 2; build phase (six to eight weeks), introducing Zone 4 intervals while maintaining Zone 2 base; peak phase (four to six weeks), maximizing Zone 4-5 intensity for performance goals; recovery phase (two to four weeks), reducing volume and intensity before the next base phase. This cycling prevents the accommodation that any constant training approach produces and mirrors the structured periodization approaches used by competitive endurance athletes. Recreational athletes applying this structure for the first time after months or years of unperiodized gray-zone training consistently report that the base phase feels boring but necessary — the discipline to do easy Zone 2 training when more intense training feels more productive is precisely the discipline that builds the aerobic foundation that makes all subsequent training more effective. Research on cardiovascular training periodization confirms superior long-term adaptation outcomes from periodized approaches compared to constant-distribution training across recreational and competitive populations.
Volume progression is the most sustainable plateau-breaking tool available for cardiovascular training — it requires no additional intensity, no new equipment, and no fundamental program change, just the commitment to spend slightly more time each week doing the cardio that is already working. The compounding effect of ten percent weekly volume additions accumulates into dramatically different fitness levels within months, producing the cardiovascular development that intensity changes alone cannot generate when aerobic base volume is the limiting factor.
Mistake 4 and 5: Post-Cardio Compensation and No Progressive Plan
Mistake 4: You Compensate for Cardio Calories Without Realizing It
Exercise increases appetite — and for many people, the caloric compensation following cardio sessions exceeds the calories burned during the session, producing a net zero or even net positive caloric balance despite regular exercise. Research on exercise and appetite consistently finds that moderate-intensity cardiovascular exercise increases food intake in many individuals by an amount partially or fully offsetting the exercise-induced caloric expenditure. This biological compensation is not a character flaw — it’s a hormonal response to energy expenditure that evolved over millions of years of caloric scarcity. It is, however, a significant reason why cardio alone rarely produces the weight loss results people expect.
The fix isn’t to stop doing cardio — cardio produces genuine cardiovascular health benefits regardless of weight change. The fix is awareness: track food intake for two weeks alongside cardio training to see whether you are unconsciously compensating. Many people find that their post-cardio eating patterns expand to fill the caloric expenditure of their training, and that awareness alone is sufficient to modify the behavior. Others find that higher-intensity training (Zone 4 to 5) produces less appetite increase than moderate-intensity training at equivalent caloric expenditure, making it more effective for weight management in individuals with strong compensatory eating responses.
Mistake 5: You Have No Progressive Plan and Are Training Without Direction
The final and most fundamental cardio mistake is the absence of a progressive plan — training sessions that accumulate time and effort without systematic progression toward a defined outcome. Without a plan, training naturally gravitates toward what is comfortable and familiar: the same distances, the same intensities, the same modalities that have always been done. Without progressive stimulus increase, fitness improvement stalls regardless of consistency.
A minimally effective progressive cardio plan requires three elements: a current fitness baseline (measured, not estimated), a specific goal (a target performance, a target heart rate at a fixed workload, a target distance at a target time), and a structured progression from current state to target state with milestones every four to six weeks. This doesn’t require sophisticated periodization — it requires deliberate planning of how training will increase over the coming weeks to ensure it always slightly exceeds current capacity. WHO physical activity guidelines recommend structured, progressive physical activity programs as superior to unplanned exercise for achieving specific health and fitness outcomes.
The Science Behind Cardio Adaptation and Why Variety Is Non-Negotiable
The human cardiovascular system adapts with remarkable precision to the specific demands placed on it — an adaptation that produces impressive fitness improvements initially and frustrating plateaus when the demands stop changing. Understanding the cellular and physiological mechanisms of cardiovascular adaptation allows you to structure training that stays ahead of the adaptation curve and continues producing results beyond the initial gains that any consistent cardio program produces.
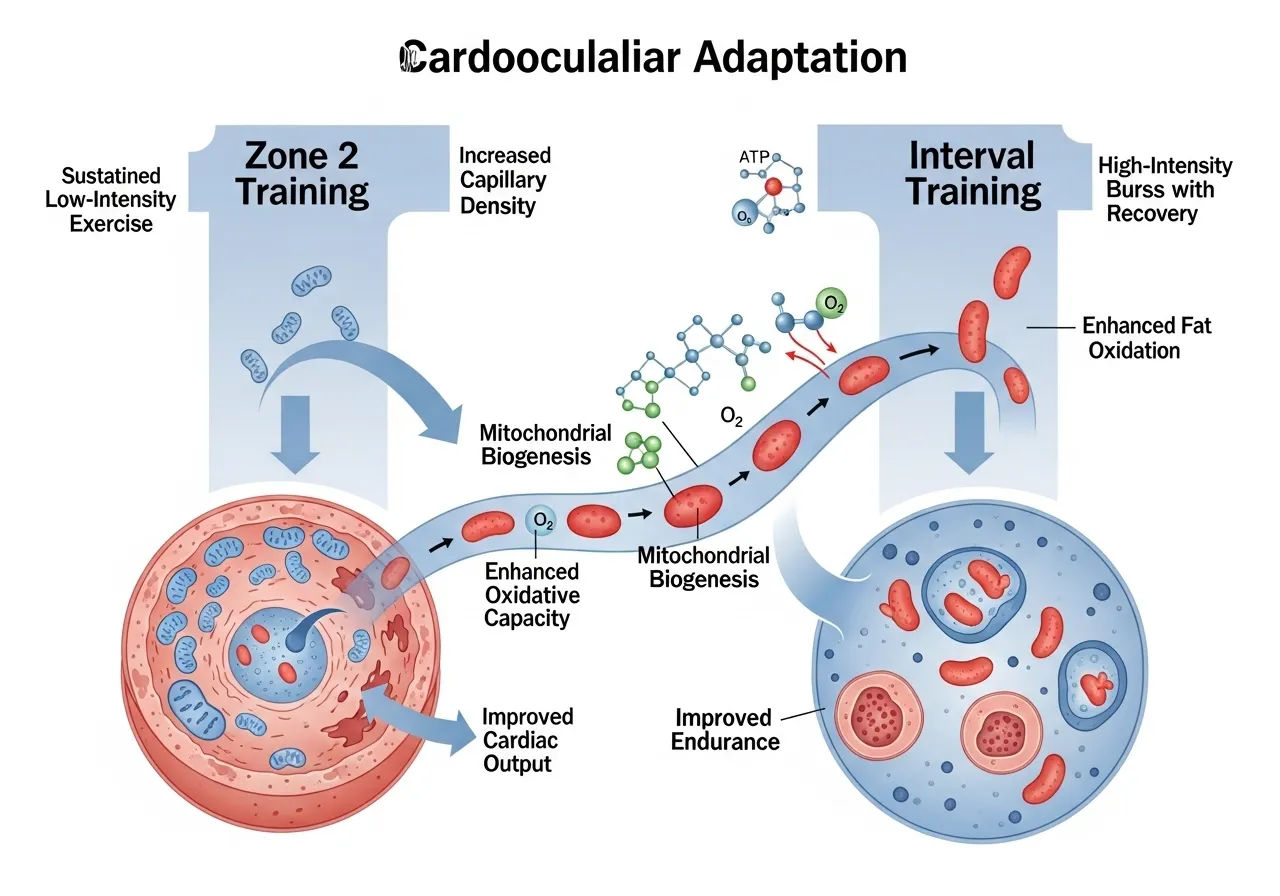
Mitochondrial Biogenesis: The Core of Cardiovascular Adaptation
The primary adaptation driving cardiovascular fitness improvement is mitochondrial biogenesis — the creation of new mitochondria within muscle cells. Mitochondria are the cellular organelles that produce ATP through aerobic metabolism, and their density within muscle tissue directly determines aerobic capacity, fat oxidation capacity, and endurance performance. Consistent cardio training at appropriate intensities triggers mitochondrial biogenesis through activation of PGC-1α, a master regulator of energy metabolism that initiates a cascade of gene expression changes resulting in new mitochondrial development over four to eight weeks of consistent training. This is why cardiovascular fitness improvements lag the start of training by several weeks — the underlying cellular changes require time to develop. Once mitochondrial density has increased to match the training demands, adaptation slows unless the training stimulus is increased or varied. Research from foundational NCBI research on exercise-induced mitochondrial biogenesis established this mechanism as the primary driver of endurance adaptation, explaining why varied training intensity is more effective than constant-load training for continued cardiovascular development.
Cardiac Remodeling: How Your Heart Changes With Training
Consistent cardiovascular training produces structural changes in the heart itself — cardiac remodeling — that improve pumping efficiency and increase maximal cardiac output. Endurance training primarily increases left ventricular volume (the amount of blood the heart can hold), allowing a larger stroke volume — more blood pumped per heartbeat — at all intensities. This is why trained athletes have lower resting heart rates than untrained people: each heartbeat delivers more oxygen, requiring fewer beats per minute to meet metabolic demands. This cardiac adaptation develops over months to years of consistent training and does not plateau as quickly as muscular adaptations, meaning cardiovascular training continues producing meaningful heart health benefits long after initial fitness plateaus are encountered. The distinction between athlete’s heart (benign cardiac remodeling from training) and pathological cardiac enlargement is well established in sports medicine and confirms that the structural heart changes produced by endurance training are health-promoting rather than harmful for virtually all exercising populations.
VO2 Max as a Plateau Indicator
VO2 max — maximum oxygen consumption per kilogram of body weight per minute — is the gold standard measure of cardiovascular fitness and plateaus after approximately six to twelve months of consistent training at the same intensity. Once VO2 max plateaus, it requires either increased training intensity, increased training volume, or novel training stimuli (such as altitude training or very high-intensity intervals) to continue improving. For recreational athletes, the five cardio mistakes described in this article — particularly same-workout repetition and gray-zone intensity — are the most common reasons VO2 max plateaus prematurely, before the individual has reached their genetic ceiling. Addressing these mistakes consistently produces VO2 max improvements of ten to twenty percent in athletes who had previously plateaued, representing major cardiovascular fitness gains achievable through programming changes alone without any additional training time. According to ACSM exercise prescription guidelines, VO2 max responds most strongly to high-intensity interval training, moderate-intensity continuous training, and appropriate periodization — the same principles that address the five cardio mistakes outlined in this article.
Action point: Estimate your current VO2 max using the Cooper 12-minute run test — run as far as possible in twelve minutes and use the formula: VO2 max = (distance in meters – 504.9) / 44.73. Retest in twelve weeks after implementing the mistake corrections described in this article. A meaningful improvement confirms the programming changes are working.
Building a Sustainable Cardio Practice T
The Cardio Science That Explains Why These Mistakes Are So Common
The five cardio mistakes are not random errors but predictable consequences of how human psychology interacts with exercise physiology. Workout repetition feels safe and familiar; variation requires discomfort with novelty. Gray-zone training feels effortful; Zone 2 feels too easy and Zone 4-5 feels genuinely hard. Insufficient volume feels like enough because sessions feel complete; more volume requires more time and discomfort. Post-cardio eating feels deserved; restraint requires countering genuine hormonal hunger signals. Training without a plan feels flexible; systematic planning requires confronting the reality of current fitness and committing to specific progressive demands. The path of least resistance in cardio training — comfortable familiar effort without systematic progression — produces the comfortable familiar results: initial improvement followed by indefinite plateau. Breaking this pattern requires the specific knowledge of why these comfortable choices produce poor physiological outcomes, and the specific alternative approaches that produce continued adaptation. This article provides both. The athlete who understands the physiology and applies the corrections has every tool needed to break through the plateau that comfortable cardio training produces and develop the cardiovascular fitness that consistent, well-structured training can genuinely create over months and years of dedicated practice. Research on exercise adherence and training behavior confirms that knowledge of training physiology significantly improves training decision quality and long-term adherence compared to effort-based training without physiological framework.
The Psychology of Cardio Plateaus: Why We Keep Doing What Doesn’t Work
The psychological pull toward familiar cardio routines is one of the strongest obstacles to breaking plateaus. Familiar routines feel safe, require less cognitive effort, and provide the comfort of known difficulty levels. Novel training approaches feel uncertain, require active attention, and carry the risk of feeling worse than the familiar approach in the short term before producing better results in the medium term. This psychological dynamic explains why most athletes who know intellectually that their cardio is not producing results continue doing the same routine — the short-term psychological cost of change feels larger than the long-term physical cost of stagnation. Breaking this pattern requires framing the change as an experiment rather than a permanent replacement — committing to try the polarized approach or the volume increase for eight weeks specifically to collect data on its effectiveness, rather than committing to change permanently without evidence. The experimental framing reduces the psychological resistance to change by making it temporary and evidence-based rather than permanent and belief-based. Eight weeks of data comparing the new approach to the previous plateau is more compelling than any argument about why the change should work, and produces the subjective experience of improvement that motivates continued application of the effective approach beyond the experimental period.
The five mistakes are correctable for every athlete at every fitness level — the corrections require knowledge and consistency, not exceptional genetics or unlimited training time. Apply them systematically, track results objectively, and experience the cardiovascular improvement that well-directed training reliably produces.
hat Produces Lifelong Results
The most sophisticated cardiovascular training program is worthless without the consistency that produces results over months and years. Building a sustainable cardio practice that survives schedule disruptions, motivational fluctuations, and the inevitable periods when training feels like a burden requires deliberate attention to the psychological and practical dimensions of exercise adherence alongside the physiological principles of cardiovascular training.
Intrinsic vs Extrinsic Motivation for Cardio
Research on exercise motivation consistently finds that intrinsic motivation — doing cardio because you find it genuinely enjoyable, because it makes you feel good, or because it is part of your identity — produces dramatically better long-term adherence than extrinsic motivation — doing cardio to lose weight, improve your appearance, or achieve specific performance metrics. Extrinsic motivation sustains training through the initial months when motivation is high and results are visible, then falters when results slow and the daily effort of training must be sustained by motivation alone. Developing intrinsic motivation requires finding cardio activities that provide genuine enjoyment, social connection, or psychological benefit beyond the physical outcomes. For some people this means finding a running group; for others it means cycling in beautiful outdoor locations; for others it means competitive events that make training meaningful beyond daily habit. The cardio activity that you will consistently choose to do for years — not the theoretically most effective modality — is the one that actually produces lifelong cardiovascular health.
Managing the Cardio-Strength Training Balance
A persistent concern among people who both lift weights and perform cardiovascular training is the interference effect — the possibility that cardio training impairs strength and muscle development. Research on concurrent training finds that this interference is real but modest and manageable. Performing cardio and strength training in separate sessions (at least six hours apart) minimizes interference compared to performing both in the same session. Favoring lower-body-intensive cardio modalities like running and cycling on lower body lifting days and upper-body-light modalities like rowing on upper body lifting days distributes the recovery demand more evenly. Limiting high-intensity cardio to two sessions per week during periods of active strength development prevents the accumulated fatigue that would otherwise compromise strength training quality. Within these practical constraints, simultaneously developing cardiovascular fitness and strength is absolutely achievable and represents the most comprehensive approach to long-term health and performance — the research concern about interference applies primarily to elite athletes trying to maximize both modalities simultaneously, not to recreational athletes pursuing moderate development of both.
Cardio for Mental Health: The Most Underrated Benefit
The mental health benefits of regular cardiovascular exercise — reduced anxiety and depression, improved cognitive function, better stress resilience, and enhanced sleep quality — are among the most robustly established findings in exercise science. Moderate-intensity cardio performed for thirty minutes three times per week produces antidepressant effects equivalent to medication in research populations with mild to moderate depression. The mechanisms include endorphin release, increased brain-derived neurotrophic factor (BDNF) that promotes neuroplasticity, reduced inflammatory markers associated with depression, and improved sleep quality that amplifies all other mental health benefits. For many people, the mental health benefits of their cardio practice are more motivating and more immediately noticeable than the physical fitness benefits, particularly in the early weeks before significant fitness changes are measurable. Recognizing and embracing these psychological benefits as primary rather than secondary training outcomes often transforms cardio from an obligatory health behavior into a genuinely valued daily practice. NCBI research on exercise and mental health confirms that regular moderate-intensity aerobic exercise is one of the most effective non-pharmaceutical interventions for anxiety and depression available in evidence-based medicine.
Action point: For the next thirty days, track not just your physical performance metrics but your mood, energy level, and sleep quality on cardio versus non-cardio days. Most people discover a clear pattern showing that cardio days produce measurably better mental states — data that becomes one of the most powerful intrinsic motivators for long-term cardio adherence.
Frequently Asked Questions About Cardio That Stops Working
How do I know if I am in the gray zone?
The gray zone is most reliably identified through heart rate monitoring — 65-80% of maximum heart rate. Without a monitor, the conversation test provides a reasonable indicator: in Zone 2, you can hold a full conversation without breath interruptions; in Zone 4-5, you can say only a few words between breaths; in the gray zone, you can speak sentences but with noticeable effort and frequent breath interruptions. Most recreational athletes who feel their cardio is working but not producing results are in the gray zone for the majority of their training time — the effort feels meaningful but the specific zone adaptations are not being developed. Confirming this through two weeks of heart rate monitoring during normal training sessions typically reveals the pattern clearly and provides the objective evidence that motivates the transition to polarized training.
Is HIIT or Zone 2 better for fat loss?
The most accurate answer is that both are necessary for optimal body composition outcomes and that neither alone produces the results that the two in combination achieve. Zone 2 training develops the fat oxidation machinery — the mitochondria and fat transport enzymes — that makes the body more efficient at using fat as fuel both during and between exercise sessions. HIIT produces the acute caloric expenditure and post-exercise metabolism elevation that maximizes total daily energy expenditure. Zone 2 alone without HIIT leaves performance ceiling development untapped; HIIT alone without Zone 2 base produces high caloric expenditure in sessions the cardiovascular system is not conditioned to recover from efficiently. The polarized combination — four Zone 2 sessions and one to two HIIT sessions per week — produces superior body composition outcomes compared to either modality alone in research comparing training approaches for recreational athletes targeting fat loss. Research on HIIT vs continuous training for body composition supports combined approaches producing superior outcomes to either modality used exclusively.
Why do I always feel hungry after cardio even when I eat beforehand?
Post-exercise hunger is driven primarily by ghrelin — a hunger hormone that increases after moderate-to-high intensity cardiovascular exercise — and by the real caloric deficit that exercise creates. These are genuine physiological hunger signals, not imagined hunger or lack of willpower. The most effective management strategies: consume 20-30 grams of protein immediately after training, which blunts ghrelin more effectively than carbohydrate or fat; time cardio sessions before planned meals rather than between meals, so the post-exercise hunger aligns with scheduled eating; and accept that some increase in appetite is appropriate and healthy after exercise, managing the amount consumed rather than trying to eliminate the hunger signal entirely. Athletes who resist post-exercise hunger without adequate nutrition compromise recovery, which impairs both the next training session and the adaptation development from the completed session — the goal is appropriate post-exercise nutrition, not post-exercise caloric restraint at the expense of recovery quality.
How do I know if my cardio plateau is from accommodation or overtraining?
Accommodation and overtraining produce opposite physiological states despite similar performance outcomes — both result in stagnant or declining performance, but require opposite interventions. Accommodation is characterized by stable resting heart rate, good energy levels, consistent performance across sessions, and stagnant improvement despite adequate training. The fix is more challenging training — higher intensity, more volume, greater variety. Overtraining is characterized by elevated resting heart rate, poor energy, inconsistent session performance, persistent soreness, and declining performance. The fix is less training — reduced volume, lower intensity, more rest. The diagnostic test: take one full week of complete rest or very light activity. If performance improves noticeably after the rest week, overtraining or accumulated fatigue was the issue, and future training should include more recovery. If performance remains flat after the rest week, accommodation was the issue, and more challenging training is needed. Most recreational athletes experiencing cardio plateaus are accommodated rather than overtrained, because the training volumes needed to produce true overtraining syndrome are higher than most recreational athletes sustain. However, high-stress life periods can create overtraining-like symptoms at lower training volumes, making the diagnostic rest week the most reliable differentiator between the two conditions.
What is the fastest way to improve cardiovascular fitness from a plateau?
The fastest legitimate improvement from a cardio plateau comes from addressing the single biggest limiting factor — which for most intermediate athletes is the Zone 2 aerobic base. Adding two Zone 2 sessions per week (twenty to thirty minutes each) to a previously stagnant training program produces measurable VO2 max improvements within four to six weeks for most people who had been training primarily in Zone 3. The second fastest improvement comes from adding one high-quality Zone 4 interval session per week — not replacing existing training but adding to it — which specifically develops lactate threshold and VO2 max ceiling simultaneously. Combining both additions (more Zone 2 base plus one quality interval session) produces the fastest legitimate cardiovascular improvement available without performance-enhancing methods, typically generating five to fifteen percent VO2 max improvement within eight to twelve weeks in previously plateaued athletes. ACSM exercise prescription for cardiovascular fitness improvement supports this combined approach as the most effective evidence-based strategy for breaking cardiovascular plateaus in recreational athletes.
Cardio that works is cardio that is specifically designed to produce the adaptations you are targeting — with the right zone distribution, sufficient volume, systematic progression, and attention to the compensation patterns that undermine results. This specificity, applied consistently, transforms cardiovascular training from a frustrating plateau into a reliable engine of measurable fitness improvement.
Frequently Asked Questions About Cardio That Stops Working
I do cardio every day. Why am I not losing weight? Daily cardio without progressive intensity variation or sufficient dietary management frequently fails to produce weight loss due to accommodation, compensatory eating, and inadequate caloric deficit. Daily Zone 2 cardio at the same intensity produces maintenance rather than change after initial adaptation. Introduce Zone 4 sessions twice weekly, measure food intake to check for compensation, and ensure total caloric intake supports the deficit required for fat loss alongside the exercise.
Should I do cardio before or after weights? For most goals, performing cardio after strength training produces better outcomes for both. Doing cardio first depletes glycogen and creates neural fatigue that reduces strength training performance. Doing cardio after strength training preserves glycogen for lifting and allows maximum strength output. The exception: if cardiovascular fitness is your primary goal and strength training is secondary, performing cardio first in a fresher state maximizes cardiovascular performance quality.
How do I know if I am overtraining with cardio? Indicators of cardiovascular overtraining include: elevated resting heart rate 5 to 10 bpm above baseline sustained over multiple days, declining performance at fixed efforts, persistent fatigue that doesn’t resolve with rest days, increased injury frequency, and disrupted sleep quality. If three or more of these are present alongside consistent high-volume training, reduce volume by 30 to 40 percent for one week and reassess. Recovery almost always produces a performance bounce that confirms the preceding fatigue was limiting progress.
My cardio fitness has improved but my weight hasn’t changed. Is cardio pointless for weight loss? No — but the mechanism requires understanding. Cardio creates caloric expenditure that supports a caloric deficit required for weight loss. If weight isn’t changing despite regular cardio, either caloric compensation is occurring (eating more to offset exercise), total caloric deficit is insufficient, or body composition is changing (muscle gain offsetting fat loss) without scale weight change. Measure body composition rather than weight alone to detect the last scenario, and track food intake to detect the first two.
Mistake 4 and 5 Advanced Analysis: Compensatory Eating and Progressive Planning
The post-cardio compensation eating pattern — consuming more calories after exercise than the exercise burned — is one of the most studied phenomena in exercise science and one of the most frustrating for athletes trying to improve body composition. Research consistently finds that exercise increases appetite proportionally to energy expenditure in most individuals, with the appetite increase often exceeding the caloric expenditure in high-intensity exercise bouts. The physiological mechanisms involve ghrelin (hunger hormone) elevation and leptin (satiety hormone) reduction following high-intensity cardiovascular exercise, creating genuine hunger signals that feel identical to the hunger that precedes actual caloric deficit. Managing this pattern requires awareness rather than willpower: eating a protein-rich meal within sixty minutes of training blunts the ghrelin response by providing satiety without excessive calories; timing cardio sessions before meals rather than before periods of high food access reduces the environmental opportunity for compensation eating; and tracking caloric intake for a week without changing eating behavior reveals the compensation pattern that most athletes underestimate or fail to notice. The athlete who addresses this compensation pattern while maintaining cardiovascular training simultaneously benefits from both the caloric expenditure of exercise and the caloric control that compensation management produces — a significantly more powerful body composition tool than either alone.
Creating a Progressive Cardio Plan That Continues Working
The fifth and most impactful mistake — having no progressive plan — produces the gradual cardio stagnation that eventually affects every athlete who trains without systematic progression. A progressive cardio plan specifies not just what to do today but how training will evolve over the next twelve to twenty-four weeks, providing the framework that ensures each week builds on the last rather than repeating it. A practical twelve-week progressive cardio plan: weeks one to four establish baseline at current fitness level, three to four sessions per week including one interval session; weeks five to eight add one additional session per week and increase interval session intensity; weeks nine to twelve add session duration and introduce a second interval session per week while maintaining Zone 2 base. This structure provides clear progression that prevents the comfortable repetition that produces accommodation, and the twelve-week timeframe allows meaningful adaptation to compound before reassessing and planning the next cycle. Twelve-week plans require four to five minutes of planning investment to write and produce twelve weeks of systematic progression — one of the highest return-on-investment planning exercises available in recreational fitness. ACSM progressive exercise programming guidelines support twelve to sixteen week planning cycles as the optimal timeframe for balancing adaptation development with program freshness across all cardiovascular fitness goals.
The Role of Cardiovascular Fitness in Overall Health and Longevity
Cardiovascular fitness — measured by VO2 max — is one of the strongest independent predictors of all-cause mortality available in medicine, stronger than body weight, blood pressure, cholesterol, or blood glucose in predicting long-term survival. Research from the Cooper Institute following tens of thousands of patients over decades found that low cardiovascular fitness was a greater mortality risk factor than smoking, obesity, or hypertension — a finding that has been replicated across multiple large population studies. The practical implication is profound: improving cardiovascular fitness through consistent training is one of the highest-impact health investments available, producing mortality risk reductions that dwarf the effect of most pharmaceutical interventions for healthy adults. Every one-MET (metabolic equivalent) improvement in cardiovascular fitness — achievable through the training approaches described in this article — is associated with approximately 13% reduction in all-cause mortality risk in population research. For the recreational athlete frustrated by a cardio plateau, this context reframes the stakes: addressing the five mistakes that stall cardio progress is not merely about running faster or feeling fitter, but about systematically improving one of the most important determinants of healthy lifespan available to proactive self-management. Landmark research from the Cooper Institute on cardiovascular fitness and mortality established the strong independent relationship between VO2 max and longevity that has been confirmed across multiple subsequent large-scale population studies.
Objective measurement of cardiovascular progress provides the feedback that guides intelligent training decisions and maintains motivation through periods of gradual improvement that subjective perception cannot detect. The most practical progress metrics for recreational cardio athletes: resting heart rate (measured first thing in the morning, declining trend indicates improving cardiovascular fitness); pace at Zone 2 heart rate (tracked monthly, improving pace at the same heart rate indicates aerobic base development); rate of perceived exertion at standardized intensities (declining RPE at the same speed indicates improved cardiovascular efficiency); and the Cooper 12-minute run test (distance covered in 12 minutes, retested every 12 weeks, provides a validated VO2 max estimate for trend tracking). These metrics, tracked consistently across months of training, reveal the gradual cardiovascular improvement that day-to-day training experience cannot perceive — the compound effect of consistent, well-directed training becoming visible only in retrospect across sufficient data points. Athletes who track these metrics report dramatically higher long-term training motivation than those who rely on subjective assessment alone, because the data reveals progress that effort-based perception misses during the inevitable slow-progress periods of cardiovascular development.
Breaking a cardio plateau requires honest assessment of which specific mistake is most responsible — accommodation, gray-zone training, insufficient volume, compensation eating, or lack of progressive planning — and targeted application of the specific correction that addresses that mistake. Generic effort increases without specific directional changes produce generic results that fail to address the specific physiological limitation driving the plateau. The athlete who applies targeted corrections with patience and consistency breaks through plateaus that untargeted effort cannot overcome regardless of its intensity.
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Exercise carries inherent risks. Always consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program, especially if you have a pre-existing medical condition, injury, or health…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…
Warning Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. The Cardio Method That Changed Everything I Thought I Knew About Training For most of my training life, I believed…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…




")










