
Hip Flexor Stretching: Why Static Stretches Alone Won’t Fix Your Tightness
This article is for general educational and informational purposes only. It does not replace professional medical or fitness advice. If you have any pre-existing condition, injury, or health concern — consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program.
Hip flexor tightness is one of the most frequently discussed complaints in fitness — and one of the most frequently mismanaged.
The standard advice is simple: stretch your hip flexors more. But for many people who stretch consistently, the tightness returns within hours and never truly resolves. If this pattern sounds familiar, the problem is likely not insufficient stretching but an incomplete approach that misses critical contributing factors.
This guide explains what hip flexor tightness actually is at a physiological level, why static stretching alone often fails to produce lasting improvement, and what a complete, evidence-informed approach looks like.
Hip Flexor Anatomy and the Physiology of Tightness
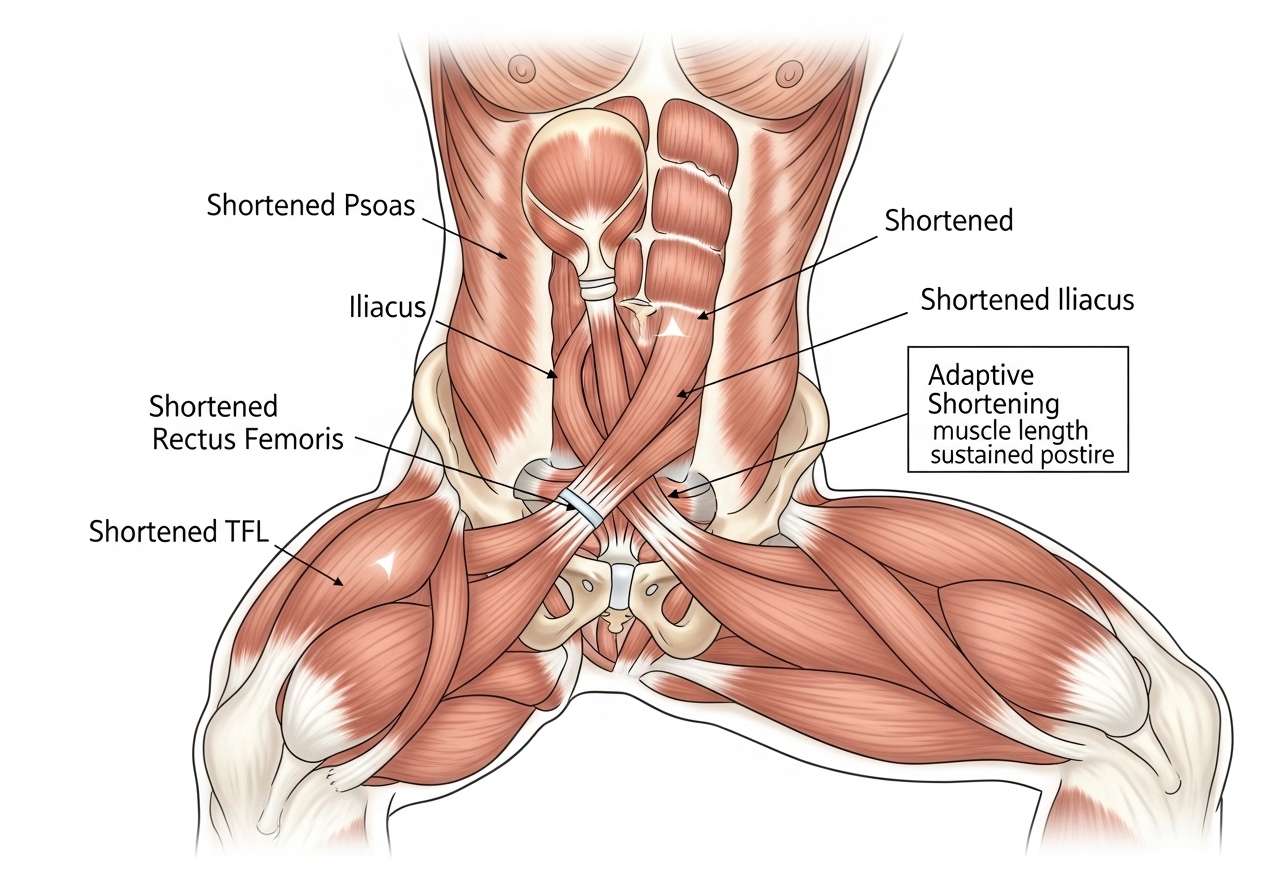
The Primary Hip Flexor Muscles
| Muscle | Attachment Points | Primary Function |
|---|---|---|
| Psoas Major | Lumbar vertebrae (L1–L5) to femur | Primary hip flexor; uniquely connects spine to leg |
| Iliacus | Iliac fossa to femur | Assists psoas in hip flexion; forms iliopsoas together |
| Rectus Femoris | Anterior hip to knee (tibial tuberosity) | Hip flexion AND knee extension — crosses both joints |
| Tensor Fasciae Latae (TFL) | Lateral hip to iliotibial band | Hip flexion, abduction, and internal rotation |
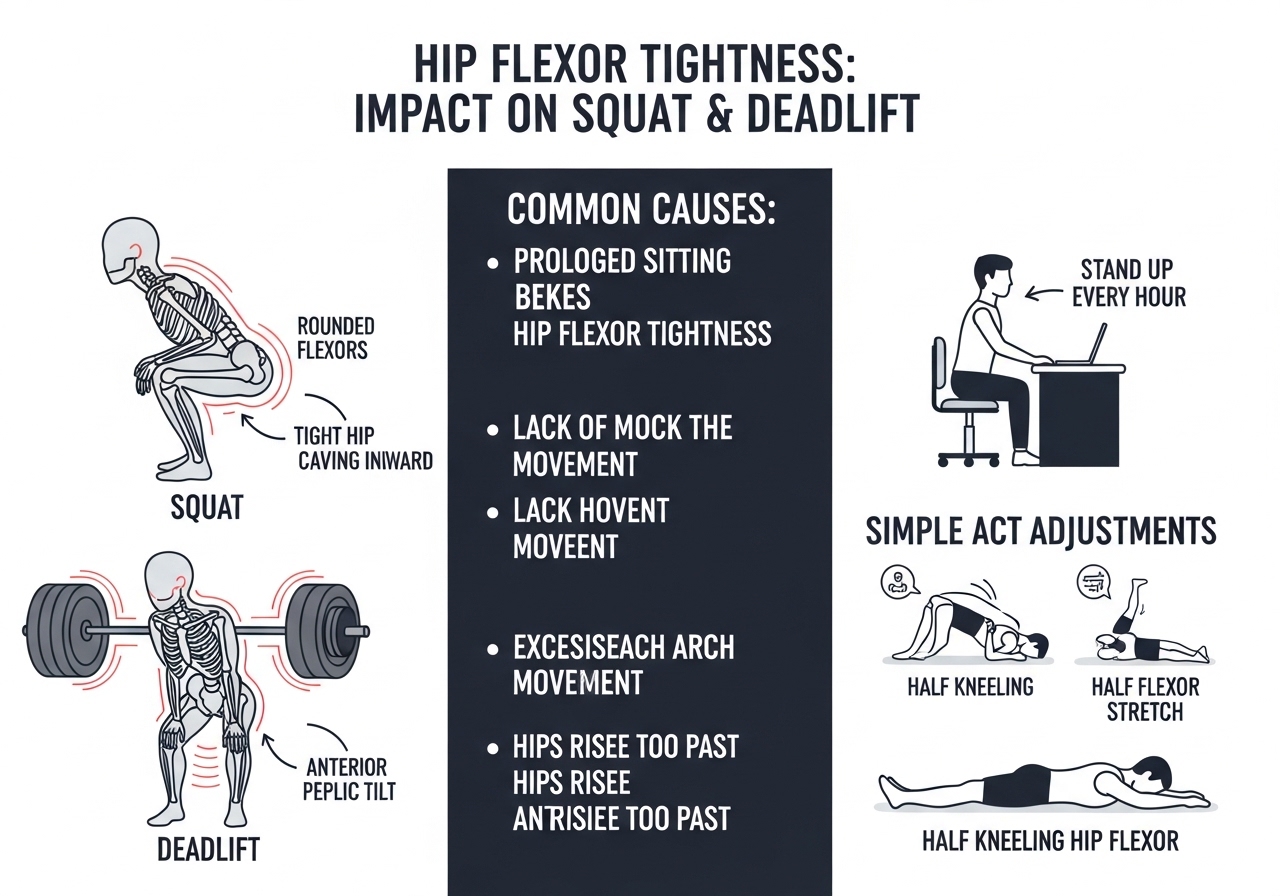
Why Prolonged Sitting Causes Tightness
When seated, the hip maintains approximately 90° of flexion. Over months and years, the hip flexor muscles may gradually lose the ability to fully lengthen into the opposite position (hip extension) — a process called adaptive shortening.
Research published in PMC found that prolonged sitting in hip flexion contributes to reduced passive hip extension range of motion, which is associated with altered movement patterns and increased injury risk during athletic and daily activities.
Two Distinct Types of Hip Flexor Tightness
This distinction is the most important concept in this guide — and the one most frequently overlooked:
| Type | Mechanism | Response to Stretching | Best Addressed By |
|---|---|---|---|
| Adaptive shortening | Muscle genuinely loses resting length from sustained shortening | Lasting improvement with consistent practice | Consistent stretching — addresses the mechanism directly |
| Neurological tone | Normal length but heightened neural activation — often from weak or inhibited glutes | Temporary relief only — tightness returns quickly | Glute activation and hip flexor strengthening through range |
Many people with chronic hip flexor tightness despite regular stretching have predominantly neurological tone rather than adaptive shortening. This is why their stretching efforts provide temporary relief but never lasting resolution — they are addressing the wrong mechanism.
The Psoas Major: Why It Deserves Special Attention
The psoas major is anatomically unique among hip flexors because it connects directly from the lumbar vertebrae (L1–L5) to the femur. A shortened or overactive psoas does not just limit hip mobility — it actively pulls on the lower spine, contributing to lumbar lordosis (the inward curve of the lower back) and potentially loading the lumbar disc and facet joints.
This anatomical reality explains why addressing psoas function sometimes produces improvements in lower back comfort — though this relationship is not universal and should not be assumed without professional assessment of the specific contributing factors in any individual case.
Self-Assessment: How to Tell if You Have Hip Flexor Tightness
Before beginning a stretching program, confirming whether hip flexor tightness is actually present provides a useful baseline and helps track progress over weeks:
1. Lie flat on a firm surface
2. Pull both knees to your chest
3. Slowly lower one leg to flat while holding the other knee to chest
4. Observe: does the lowered thigh lift off the surface before the leg is fully extended?
A clearly lifting thigh suggests hip flexor tightness on that side
Note: self-assessment has limitations — a physiotherapist can perform more accurate clinical testing, distinguish between muscle shortening and other types of restriction, and assess whether the degree of tightness is clinically relevant for your specific situation and goals.
Hip Flexors and Breathing
The psoas major’s attachments to the lumbar vertebrae place it in anatomical proximity to the diaphragm (the primary breathing muscle, which also attaches to the lumbar spine). Some physiotherapists include diaphragmatic breathing practice in hip flexor and lower back rehabilitation programs based on proposed shared fascial and mechanical relationships.
Learning diaphragmatic breathing — breathing into the belly rather than the chest — is a low-risk practice that is widely included in clinical mobility programs. A simple daily practice: lie on your back, place one hand on chest and one on belly, breathe so only the belly hand rises for 5 minutes. Whether the mechanism is primarily fascial, neurological, or psychological, this practice consistently appears in clinical mobility programs and carries minimal risk for most individuals.
Hip Flexor Tightness in the Context of Chronic Pain Research
The relationship between hip flexor muscle length, tone, and chronic pain is more complex than popular fitness content typically suggests. Research examining this relationship shows mixed findings — some studies find strong correlations between hip flexor tightness and lower back pain, while others find weak or no association when confounding variables are controlled.
This does not mean hip flexor work is not valuable — it means the claim that “tight hip flexors cause lower back pain” should be understood as a possible contributing factor in some individuals rather than a universal causative relationship. A healthcare professional can assess whether hip flexor function is a meaningful contributor to any specific pain presentation you are experiencing.
This assessment is the critical starting point.
Why Static Stretching Alone Often Fails to Resolve Hip Flexor Tightness
The Temporary Relief Pattern
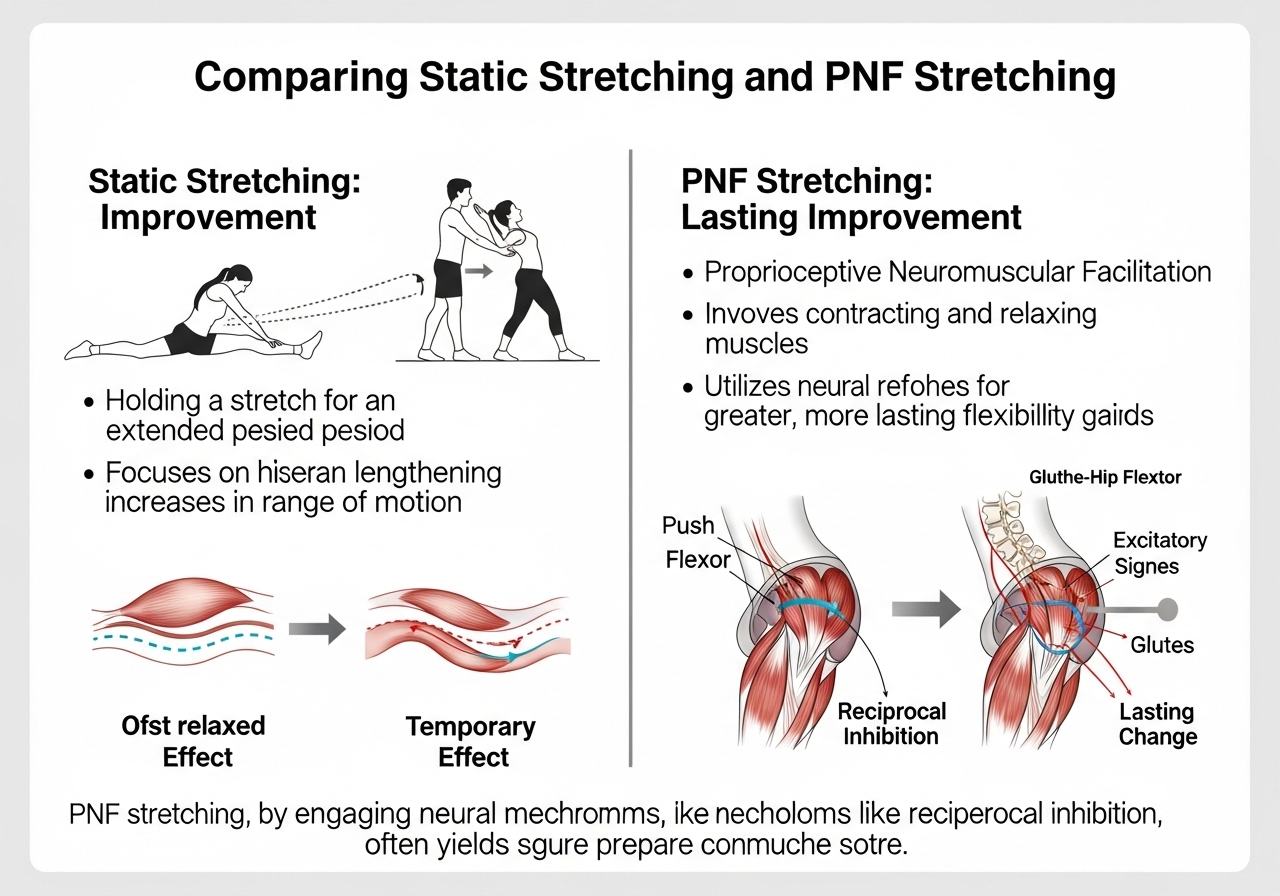
Static stretching (holding a muscle in a lengthened position for 30 seconds or longer) reliably increases range of motion in the short term — range typically improves immediately after the stretch is performed.
For many people with chronic hip flexor tightness, however, this improvement disappears within hours and the feeling of tightness returns. This pattern strongly suggests a neurological mechanism that static stretching does not directly address.
What the Research Shows
A systematic review and meta-analysis published in PMC examining the influence of hip flexor stretching on performance parameters found that static hip flexor stretching produced performance impairments of 3.7–4.4% when performed immediately before physical activity. This means static stretching of the hip flexors should be placed post-training or in a dedicated mobility session — not immediately before training or competition where performance is needed.
This finding does not mean static stretching is ineffective. It means the timing and context of stretching significantly affect outcomes.
Reciprocal Inhibition: The Glute Connection
Reciprocal inhibition is a fundamental neurological principle: when one muscle contracts, its direct antagonist (the muscle that performs the opposite movement) receives neural inhibition to allow smooth movement.
The hip flexors and gluteus maximus are antagonists — the glutes extend the hip, the hip flexors flex it.
When the glutes are chronically weak or inhibited from prolonged sitting — extremely common in desk-working populations — the hip flexors may remain in a state of elevated neural tone as a compensatory pattern to maintain hip stability.
This is the missing piece that explains why stretching-only approaches fail for many individuals: without activating and strengthening the glutes, the neurological driver of the elevated tone remains unaddressed regardless of how consistently the hip flexors are stretched.
PNF Stretching: A More Effective Technique
Proprioceptive Neuromuscular Facilitation (PNF) stretching involves contract-relax cycles that consistently outperform passive static holds in research on range of motion improvement.
A study published in PMC comparing stretching techniques for iliopsoas flexibility found that PNF technique produced more pronounced improvements in hip flexor flexibility and range of motion compared to standard static stretching approaches — supporting contract-relax methods as a superior option for many individuals.
Basic PNF protocol for hip flexors:
Step 2: Gently press the back knee into the floor — approximately 20–30% effort for 6–8 seconds
Step 3: Completely relax, then actively move to a slightly deeper stretch position
Step 4: Hold the new position for 20–30 seconds
Repeat: 2–3 cycles per side
Timing Hip Flexor Work With Training
A practical weekly schedule for integrating hip flexor work with regular training:
Dynamic mobilization: leg swings × 15, hip circles × 10, walking lunges × 8
Training days — after session (5 min):
Kneeling lunge stretch × 2 each side (30 sec) + Glute bridge 2 × 15
Non-training days — morning or evening (12–15 min):
Full 3-phase protocol: kneeling lunge + couch stretch + PNF + glute activation + hip flexor strengthening
This structure provides daily attention without requiring a dedicated session every training day. The intensive 3-phase protocol falls on rest days when there is no competing training fatigue or time pressure.
Understanding Why the Tightness Returns
For many people who have stretched consistently without lasting results, the pattern of temporary relief followed by return of tightness within hours is both frustrating and informative. This pattern itself is diagnostic: it strongly suggests that the mechanism is neurological (elevated tone from glute inhibition or compensatory patterns) rather than structural shortening — because structural shortening does not reverse itself within hours of a stretch session and then return when the stretch is removed.
Recognizing this pattern is the first step toward a more effective approach. Rather than stretching more frequently or more intensively, the productive intervention is to address the neurological driver — which means glute activation and hip flexor strengthening through range, not simply more sustained passive holds.

The Complete 3-Phase Hip Flexor Protocol
Phase 1 — Stretching: Three Essential Variations
1. Half-Kneeling Hip Flexor Stretch (Primary)
The most widely prescribed hip flexor stretch — but only effective when performed with the posterior pelvic tilt detail that most instructors omit:
Critical cue — the posterior pelvic tilt: Before shifting forward, actively squeeze the back-leg glute and tuck the pelvis slightly backward. Without this tilt, the body compensates by arching the lower back instead of actually stretching the psoas.
Duration: 30–45 seconds × 3 sets each side | Daily for improvement
The pelvic tilt detail is what distinguishes a genuine psoas stretch from a lower back arch. Research comparing stretching techniques confirmed that a stretch incorporating posterior pelvic tilt produced significantly greater hip extension range of motion improvement than a standard hip extension stretch without pelvic positioning control.
2. Couch Stretch (Rectus Femoris)
Target: Specifically the rectus femoris — the quad muscle crossing both hip and knee that standard lunge stretches significantly undertarget
Duration: 30–45 sec × 2–3 each side
⚠️ Avoid if knee pain occurs in this position
3. Standing Hip Flexor Stretch (PNF Version)
The standing version of the kneeling lunge stretch using the PNF contract-relax protocol described in the previous section — appropriate once the kneeling version has been practiced for 2+ weeks and the pelvic tilt cue is reliably executed.
Phase 2 — Glute Activation
Performing glute activation exercises immediately before or after stretching addresses the neurological tone component that stretching alone cannot resolve:
Exercise 2 — Clamshells: 2 × 15 each side | Controlled rotation, avoid letting the pelvis rock
Exercise 3 — Side-Lying Hip Abduction: 2 × 15 each side | Keep toes pointed forward, not upward
Exercise 4 — Prone Hip Extension: 2 × 10 each side | The glute initiates the movement — not the lower back
Phase 3 — Hip Flexor Strengthening Through Range
The third phase is the most commonly omitted — and often the most important for people with neurological tone. Muscles that are weak at end range often feel “tight” because the nervous system restricts movement into positions it cannot control under load.
Strengthening the hip flexors through their full range signals the nervous system that these positions are safe and controllable:
- Hanging Knee Raises: 3 × 10 — active hip flexion through the full available range
- Standing Banded Hip Flexion: 3 × 12 each side — controlled eccentric lowering
- Dead Bug (Psoas March variation): 3 × 8 each side — hip flexion against core stability demand
4-Week Daily Practice Plan
| Week | Daily Practice (10–15 min) | Expected Outcome |
|---|---|---|
| 1 | Kneeling stretch × 3/side (30 sec) + Glute bridge 2 × 15 | Initial relief; glute-hip flexor pattern begins activating |
| 2 | Add couch stretch + clamshells 2 × 15 each side | Rectus femoris beginning to lengthen |
| 3 | Add hanging knee raises or banded hip flexion 3 × 10 | Active strength through full hip flexion range developing |
| 4 | Full protocol 4–5 days/week; assess squat and lunge quality | Measurable improvement in hip extension range |
Lasting improvement typically requires 6–12 weeks of consistent daily practice — not 1–2 weeks. If no measurable improvement occurs after 8 weeks of consistent daily work, a physiotherapist assessment may identify whether a different mechanism (joint restriction, scar tissue, or a specific neural cause) is the limiting factor.
Foam Rolling as a Preparation Tool
Foam rolling the TFL (lateral hip area) and anterior hip for 60–90 seconds per side before stretching may reduce the sensation of tightness enough to allow a more comfortable and productive stretch position. The proposed mechanism is neurological — reducing motor drive to the muscle temporarily — rather than mechanical tissue lengthening.
As a preparation tool before stretching, not as a replacement for it, lateral hip and TFL foam rolling is a practical addition that many trainees find helpful. Applying direct foam roller pressure to the psoas itself is uncomfortable and not recommended — the kneeling lunge stretch and PNF approaches are more appropriate interventions for this muscle.
Progression Beyond the 4-Week Plan
After completing the initial 4-week daily practice plan, maintaining and building on the progress achieved requires transitioning from an intensive daily protocol to a sustainable maintenance approach:
- Weeks 5–8: Continue full protocol 4–5 days per week — most people see the clearest range improvements in this period as the neurological and structural changes consolidate
- Weeks 9–12: Reduce to 3–4 days per week if improvement is maintained — assess squat and lunge quality to confirm that range is being utilized functionally
- Maintenance (month 4+): 5–8 minutes of daily light stretching and glute activation preserves the gains that required 10–15 minutes to build
Hip Flexor Tightness: Effects on Training Performance and Daily Movement
Impact on Resistance Training
Hip flexor tightness most commonly manifests in resistance training as movement restriction at specific ranges:
- Squat: Excessive forward torso lean in the bottom position, or the hips shooting back faster than the chest rises on the ascent — both driven by limited hip extension at the top requiring compensation elsewhere
- Deadlift: Difficulty maintaining the hip hinge position at setup, or the lower back rounding earlier in the pull than hamstring flexibility alone would explain
- Lunge: A pulling or aching sensation in the front of the hip on the back leg, reduced comfortable stride length, or the pelvis tilting anteriorly during the movement
Anterior Pelvic Tilt and Its Effects
Overactive or shortened hip flexors may contribute to anterior pelvic tilt (the pelvis tipping forward, which increases the lumbar curve). This position:
- Increases compressive loading on the lumbar facet joints (the small posterior joints between vertebrae)
- Places the gluteus maximus at a mechanical disadvantage, reducing its ability to generate hip extension force
- May contribute to chronic lower back aching — particularly noticeable during prolonged standing
It is important to note that some degree of anterior pelvic tilt is entirely normal — the question is whether it is excessive and whether it is contributing to specific movement limitations or discomfort. This determination requires professional assessment and should not be self-diagnosed.
Lifestyle Factors That Perpetuate Tightness
Ten minutes of daily stretching cannot fully offset 8–10 hours of sustained hip flexion in seated positions. Lifestyle adjustments significantly reduce the cumulative adaptive shortening that drives tightness:
- Hourly standing breaks: Standing and walking for 2–3 minutes every 45–60 minutes of sitting interrupts sustained hip flexor shortening throughout the day
- Standing desk periods: Alternating between sitting and standing during desk work — not standing all day, which creates different postural demands
- Sleep position: Habitual side-sleeping in a heavy fetal position (knees drawn toward chest) maintains hip flexors shortened for hours overnight — a pillow between the knees to maintain a more neutral hip position may help some individuals
When Hip Flexor Stretching May Not Be the Right Approach
A clinically documented and counterintuitive scenario: some individuals presenting with hip flexor “tightness” actually have hip flexors that are lengthened and overused — not shortened and tight. In these cases, additional stretching worsens symptoms by further stressing already-elongated tissue.
Warning signs that the mechanism may not be shortening:
- Pain or burning specifically at the hip flexor during the stretch (not just a pulling sensation)
- Snapping or clicking in the front of the hip during movement — a possible sign of snapping hip syndrome (coxa saltans)
- Symptoms consistently worsening over multiple weeks of stretching practice
Any of these presentations warrants evaluation by a physiotherapist before continuing a stretching program.
Common Questions About Hip Flexor Stretching
How do I know if my hip flexors are actually tight?
The Thomas Test provides a useful clinical indicator: lie flat on a firm surface, pull both knees to your chest, then slowly lower one leg back to flat while holding the other knee to chest. If the lowered thigh lifts significantly off the surface before the leg is fully extended, this suggests hip flexor tightness on that side. A physiotherapist can perform more accurate testing and distinguish between muscle shortening and other types of restriction.
Should I stretch before or after training?
Before training: dynamic hip flexor mobilization only — controlled leg swings, walking lunges, hip circles (15–20 reps each). Static holds before training may temporarily reduce strength output by 3–4%. After training: static stretches held for 30–45 seconds are appropriate — the muscle is warm, injury risk is lower, and no subsequent performance demand will be affected. Dedicated morning or evening sessions (10–15 minutes of the full 3-phase protocol) are the most effective format for addressing chronic tightness.
Can tight hip flexors cause lower back pain?
Tight or overactive hip flexors may contribute to lower back pain in some individuals — particularly through the anterior pelvic tilt and psoas tension mechanisms described above. However, lower back pain is caused by many factors, and attributing it to hip flexors without proper assessment often leads to ineffective treatment. If you have lower back pain, consulting a licensed physiotherapist or sports medicine physician for an accurate diagnosis is strongly recommended before beginning a self-directed stretching program.
- Static stretching alone often fails for chronic tightness — the mechanism may be neurological, requiring glute activation and hip flexor strengthening, not just more stretching
- The posterior pelvic tilt cue in the kneeling lunge stretch is the single most important technical detail for stretching the psoas rather than compensating through lumbar arch
- PNF contract-relax stretching produces greater and more lasting range of motion improvements than passive static holds
- Lasting improvement requires 6–12 weeks of consistent daily practice — not occasional stretching
- Symptoms that worsen with stretching, or no improvement after 8 weeks, warrants physiotherapist evaluation
Hip Flexor Considerations for Resistance Training Populations
For intermediate and advanced strength trainees, hip flexor restrictions commonly limit performance in specific exercises rather than being felt as a distinct sensation of tightness:
- Powerlifters: Hip flexor restriction at the top of the squat and deadlift creates compensatory lower back extension — addressing hip flexor mobility may directly improve the ability to maintain optimal spinal position at lockout
- Olympic weightlifters: The receiving position in the clean and snatch requires full hip extension during the drive phase — hip flexor restriction limits the force production window
- Bodybuilders: Hip flexor tightness distorts pelvic position during leg press, RDL, and hip thrust — reducing the effective range of motion for the target muscles
In each case, addressing hip flexor mobility produces direct performance improvements rather than just improving the sensation of tightness — making it a performance intervention as much as a comfort and injury prevention practice.
Understanding and correctly identifying which mechanism is present is therefore the essential first step that determines the most effective treatment strategy.
Long-Term Hip Flexor Practice: Sport Applications, Aging, and Sustainable Maintenance
Sport-Specific Applications
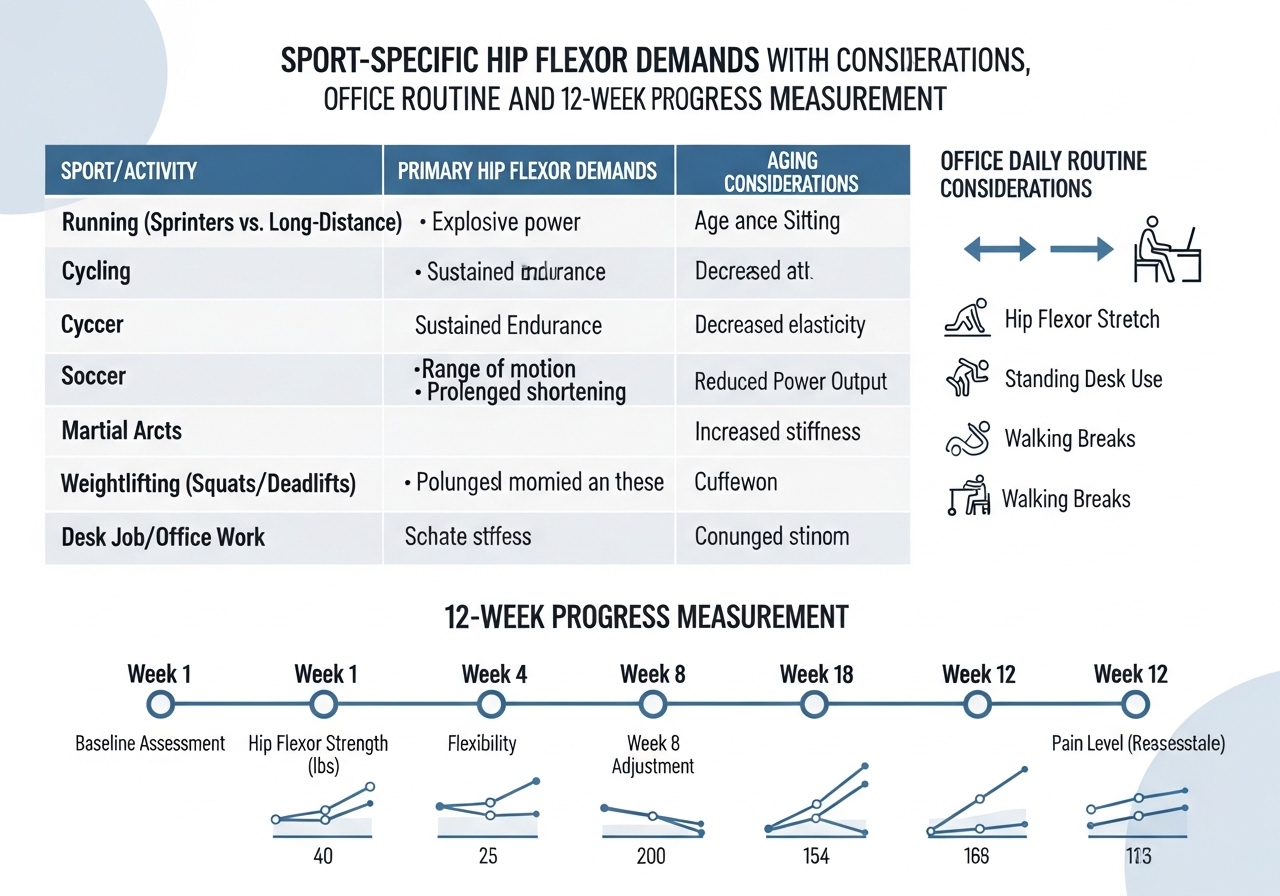
| Sport | Hip Flexor Demand | Priority Approach |
|---|---|---|
| Running / Sprinting | Full hip extension range needed for stride length and power | Daily kneeling lunge stretch + active hip extension drills |
| Cycling | High hip flexor use; sustained shortening during rides | All three stretches + daily glute activation |
| Olympic Lifting / CrossFit | Deep squat requires full hip extension at top of lifts | Couch stretch + hip flexor strengthening through range |
| Martial Arts | Dynamic hip flexion and extension in kicking and grappling | PNF stretching + active range of motion work |
Hip Flexor Mobility and Aging
Hip flexor flexibility commonly declines with age — particularly for individuals who become more sedentary. For older adults (60+), hip flexor tightness may contribute to reduced walking stride length and speed, difficulty rising from low chairs, increased lower back discomfort during prolonged standing, and reduced balance during single-leg activities.
A gentle version of the kneeling lunge stretch and regular glute bridge work is appropriate for many older adults. However, all exercise programming for adults with joint conditions, osteoporosis, or balance concerns should be directed by a qualified healthcare provider or exercise physiologist to ensure safety.
The Office Worker’s Daily Protocol
For individuals who sit for 6+ hours daily, a minimal but consistent daily routine may prevent progressive tightness from accumulating:
✅ Stand and perform 10 hip circles each direction
✅ Half-kneeling stretch with posterior pelvic tilt — 30 sec each side
✅ 15 standing glute squeezes — feet hip-width, actively contract glutes
✅ 10 standing hip extension pulses each side
This minimal routine, performed twice daily during work hours, interrupts the sustained shortening that sitting produces throughout the day — significantly reducing the amount of recovery work the evening stretching session needs to accomplish.
Measuring Progress Over 12 Weeks
| Assessment | Method | Expected Change (8–12 weeks) |
|---|---|---|
| Kneeling lunge depth | Side photo — distance front shin travels forward | Measurable increase before lumbar compensation begins |
| Squat quality | Side video — torso lean angle at bottom | Reduced anterior lean, improved depth |
| Tightness rating | 1–10 subjective score at start of each session | Gradual decline from initial baseline |
Monthly review of these indicators often reveals improvement that daily practice makes difficult to perceive. The gradual nature of flexibility change is the main reason consistent daily practice over months outperforms intensive periodic sessions.
Building a Sustainable Long-Term Practice
The individuals who successfully resolve chronic hip flexor tightness virtually all share the same characteristic: they committed to a daily practice for at least 8–12 weeks without expecting rapid resolution, and they addressed both the stretching and the activation components — not stretching alone.
Viewing hip flexor mobility work as a permanent health practice — like brushing teeth — rather than a temporary fix for current discomfort produces lasting outcomes for most people who have previously cycled through improvement-then-regression patterns.
Once initial tightness is resolved through consistent daily practice, maintenance requires significantly less time than the building phase — typically 5–8 minutes of daily light stretching and glute activation maintains the improvement that took 10–15 minutes of daily dedicated work to develop. A qualified physiotherapist can provide personalized guidance if self-directed efforts plateau or if specific clinical factors are contributing to the tightness.
Hip Flexor Stretching After Lower Body Training
A brief post-session hip flexor stretch (kneeling lunge, 2 × 30 seconds each side) immediately after lower body training may help prevent the post-session tightening that occurs as muscles cool and training-related fatigue metabolites accumulate. Keep the intensity gentle during this period — muscles are fatigued and aggressively forcing range immediately after heavy squats or deadlifts may increase soreness rather than reduce it.
Professional Support: When to Seek It
Self-directed hip flexor work is appropriate and effective for most healthy adults. Professional support adds significant value in specific situations:
- No improvement after 8 weeks of consistent daily practice — a different mechanism may be limiting progress
- Pain during stretching rather than just a pulling sensation — not normal, warrants assessment
- Associated lower back pain that does not respond to the protocol — multiple contributing factors may be present
- Returning to training after hip flexor strain or surgery — professional guidance for the return-to-loading progression is strongly recommended
A qualified physiotherapist can assess the dominant mechanism of tightness, prescribe a protocol specifically matched to your individual anatomy and goals, and identify any clinical factors that require specific intervention beyond a general flexibility program.
In all cases, the combination of patience over a meaningful time horizon — 8 to 12 weeks at minimum — with an approach that addresses all three components of the problem (stretching, glute activation, and active hip flexor strengthening through range) produces the most consistent and lasting outcomes across different populations, training backgrounds, and tightness severities. Across all presentations of hip flexor tightness — whether predominantly structural, neurological, or a combination of both — the three-phase approach of stretching, glute activation, and hip flexor strengthening through range provides a comprehensive intervention framework that addresses all the most common contributing mechanisms simultaneously.











