
Rectus Femoris Guide: Why This Two-Joint Muscle Causes Anterior Knee Pain, Limited Squats, and Running Restrictions
The rectus femoris is the quadriceps muscle that crosses two joints rather than one. While the vastus lateralis, vastus medialis, and vastus intermedius cross only the knee, the rectus femoris originates at the anterior inferior iliac spine of the pelvis and crosses both the hip and the knee. This two-joint architecture means the rectus femoris can be limited by either hip extension range or knee flexion range independently, and when it tightens — as it does in virtually everyone who sits for extended periods — it creates restrictions and compensations at both joints simultaneously.
A tight rectus femoris affects three domains simultaneously. At the knee, it increases the tension on the patellar tendon and the compressive load on the patellofemoral joint, contributing to the anterior knee pain presentations that include patellofemoral pain syndrome, patellar tendinopathy, and Osgood-Schlatter disease in adolescents. At the hip, it limits hip extension range during the late stance phase of walking and running, forcing compensatory anterior pelvic tilt and increased lumbar extension to achieve the stride length the limited hip extension cannot provide. In loaded squatting, it creates the early heel rise, forward trunk lean, and limited depth that characterise the trainee who looks like they are falling forward as they approach parallel.
This guide covers the anatomy and two-joint mechanics of the rectus femoris, what the research shows about rectus femoris tightness and knee pain, how to assess whether the rectus femoris is the limiting factor in your specific presentation, beginner through advanced stretching and strengthening protocols, and how to address the compensation patterns that prolonged rectus femoris tightness creates in the hip and lumbar spine.
Why Is the Rectus Femoris Different From the Other Quad Muscles, and Why Does That Matter?
The Structural Basis of the Double-Joint Problem
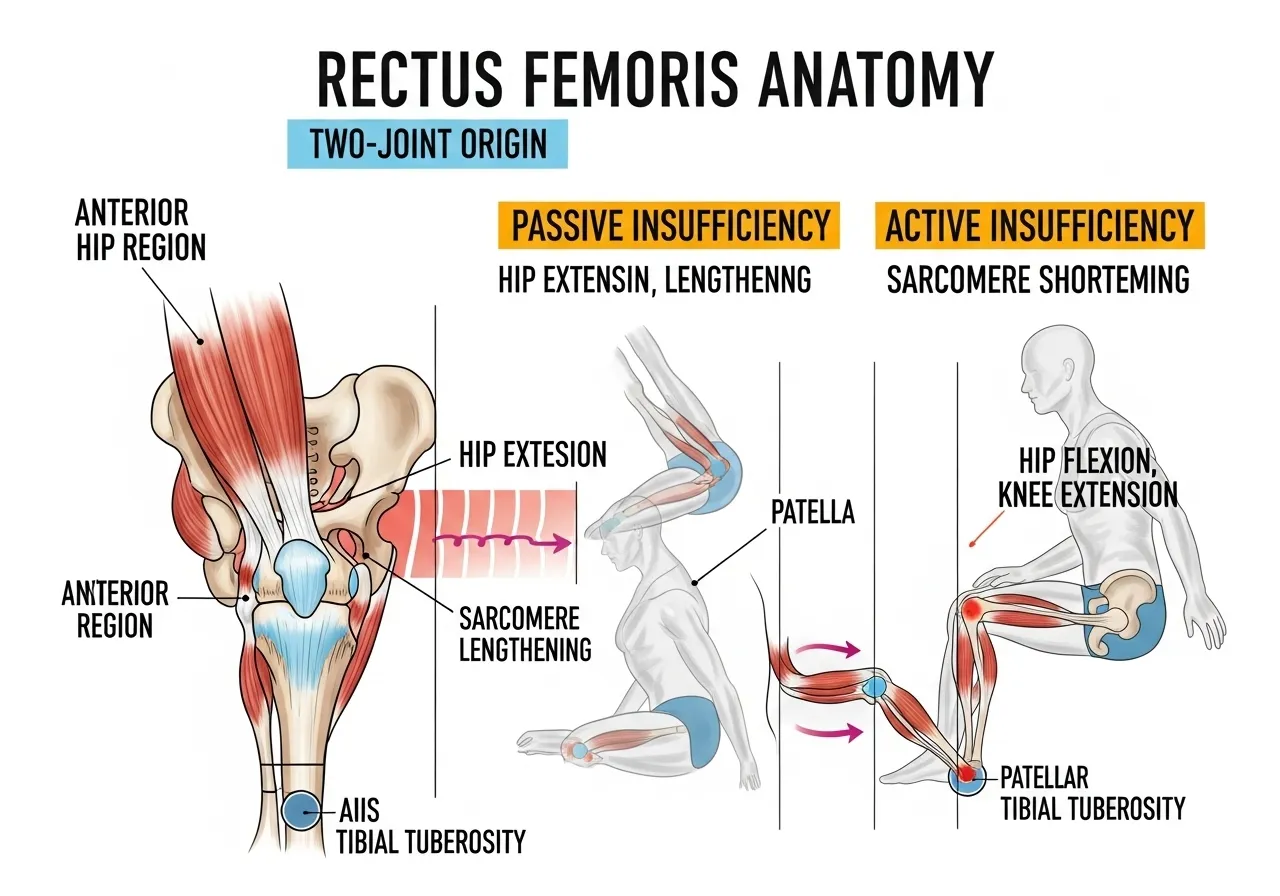
The rectus femoris runs from the anterior inferior iliac spine (AIIS) of the pelvis, across the hip joint’s anterior aspect, down the anterior thigh, and inserts through the quadriceps tendon into the patella and then through the patellar tendon into the tibial tuberosity. This continuous tendon-bone pathway means that shortening of the rectus femoris muscle creates simultaneous tension at both its proximal (hip) and distal (knee) attachments.
When the hip is in extension and the knee is in flexion simultaneously — the combination that characterises the late swing phase of running, deep squatting, and the kneeling position — the rectus femoris must lengthen at both ends simultaneously. For a muscle that has adapted to the shortened, hip-flexed, knee-extended position of sitting, this combined lengthening demand exceeds the available range and produces the characteristic tight-rectus-femoris compensations: anterior pelvic tilt to reduce the hip extension demand, reduced knee flexion to limit the distal stretch, or early heel rise to shorten the overall limb length and reduce the combined stretch.
Passive vs Active Insufficiency in the Rectus Femoris
The rectus femoris’s two-joint architecture creates two insufficiency phenomena. Passive insufficiency occurs when the muscle is too short to allow the joints it crosses to move to their full range simultaneously — the hip cannot fully extend while the knee is flexed, or the knee cannot fully flex while the hip is extended, because the muscle’s length limits both. Active insufficiency occurs when the muscle is so lengthened across both joints simultaneously that it cannot generate adequate force — the rectus femoris cannot maximally extend the knee when the hip is also in maximal extension because it is already stretched to near its maximum useful length.
The Sitting Position as the Primary Tightening Mechanism
Prolonged sitting maintains the rectus femoris in a shortened position: the hip is flexed, reducing the tension on the proximal muscle attachment, and the knee is flexed, reducing the tension on the distal attachment. Over months and years of prolonged sitting, the rectus femoris adapts to this shortened length through sarcomere loss — the contractile units within each muscle fibre decrease in number as the muscle adapts to the habitual shortened length. This sarcomere loss reduces the muscle’s resting length and its available extensibility, which is why releasing a tight rectus femoris requires not just acute stretching but sustained work over weeks to months to restore sarcomere number and functional muscle length.
The Anterolateral Hip Pain Connection
Rectus femoris tightness contributes to anterolateral hip pain and what is sometimes misdiagnosed as hip impingement. The tight rectus femoris creates abnormal tension at its proximal attachment at the AIIS, which can produce a localised anterior hip pain that mimics hip labral pathology and true femoroacetabular impingement. The distinction is clinically important: the anterior hip pain from rectus femoris proximal attachment tension is soft tissue in origin and responds to targeted stretching and massage at the AIIS region. True FAI involves bony pathology that requires different management. The hallmark of the rectus femoris proximal attachment pain is that it reproduces with direct palpation at the AIIS and with the combined hip extension and knee flexion position (modified Thomas test position) that stretches the rectus femoris maximally.
Rectus Femoris and Running Economy
The hip extension limitation that tight rectus femoris creates during running has direct effects on running economy. Adequate hip extension during late stance phase is essential for effective elastic energy storage and return in the posterior kinetic chain. When the rectus femoris limits hip extension, the late stance phase propulsion is reduced, the stride length decreases, and the lumbar spine compensates by extending further to allow the perceived forward propulsion to continue. This lumbar compensation in high-mileage runners contributes to the lumbar pain and hip flexor strain patterns that are disproportionately common in desk-based recreational runners whose hip extension is limited by occupational sitting.
Research: Rectus Femoris Tightness and Anterior Knee Pain
PFPS and Rectus Femoris Tightness: Cross-Sectional Evidence
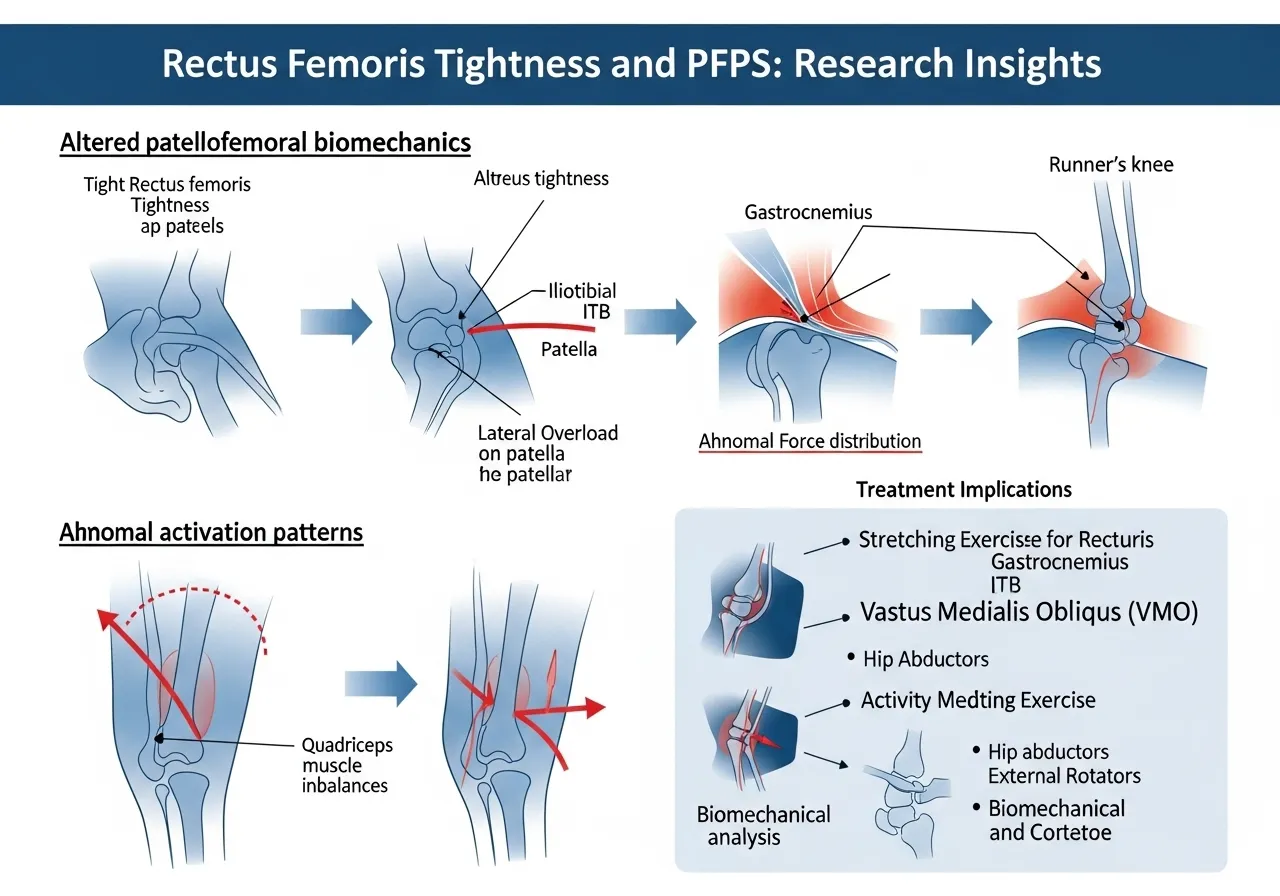
A study examining the association of patellofemoral pain syndrome with quadratus lumborum and lower limb muscle tightness found that PFPS was associated with tightness of rectus femoris, gastrocnemius, and iliotibial band, with no association found between hamstring and quadratus lumborum tightness and PFPS, confirming that rectus femoris tightness is a clinically relevant factor in patellofemoral pain syndrome presentations and suggesting that flexibility assessment and intervention targeting the rectus femoris should be included in the management of anterior knee pain alongside the patellar tracking and quadriceps strengthening interventions that dominate standard rehabilitation protocols.
Rectus femoris tightness is significantly associated with PFPS. Targeted rectus femoris flexibility intervention should be part of anterior knee pain management, not just patellar tracking exercises and VMO strengthening, which are typically the sole focus of standard PFPS rehabilitation.
Anterior Knee Pain Biomechanics: The Patellofemoral Stress Mechanism
A review examining patellofemoral pain rehabilitation from a biomechanical perspective found that alterations in force vectors due to muscular imbalance, soft-tissue tightness or laxity, and altered functional movement patterns can all combine to create a painful anterior knee, and that this movement pattern results in disproportionate loading of the lateral patellofemoral joint reducing patellofemoral contact area and increasing focal joint stress, with muscular tightness of the lateral structures including the rectus femoris and iliotibial band contributing to the abnormal patellar tracking that produces the patellofemoral compression and shear forces underlying anterior knee pain.
Muscular tightness including rectus femoris contributes to abnormal patellar tracking and lateral patellofemoral joint overload. Soft-tissue tightness is one of several interacting factors in PFPS, alongside hip weakness, patellar alignment, and movement pattern alterations.
Rectus Femoris and Running: Muscle Activation in Runners With PFPS
A study examining bioelectrical activity of vastus medialis and rectus femoris muscles in recreational runners with anterior knee pain found that the decrease in the median frequency of vastus medialis and rectus femoris muscles was significantly greater in runners with PFPS in comparison to the control group, confirming that altered muscle activation patterns in the quadriceps complex, including changes in rectus femoris muscle behaviour, are associated with patellofemoral pain syndrome in recreational runners and that targeting the biomechanical and muscular factors contributing to altered quadriceps activation represents a comprehensive approach to PFPS management in running athletes.
Rectus femoris muscle activation changes characterise PFPS in recreational runners. Both structural tightness and functional activation patterns of the rectus femoris contribute to patellofemoral pain, requiring both flexibility and activation-pattern interventions for comprehensive management.
The Knee Flexion Angle at Which Rectus Femoris Tightness Matters Most
Rectus femoris contribution to patellar compression is greatest at 30 to 60 degrees of knee flexion, where the muscle’s moment arm at the knee is longest relative to the patella’s position in the femoral trochlear groove. At this range — which corresponds to the mid-range of stair descent, the start position of a squat, and the knee flexion during single-leg landing — a tight rectus femoris generates elevated patellar compression force that stresses the articular cartilage and the subchondral bone of the patellofemoral joint. This specific vulnerability window explains why PFPS pain is characteristically worst during stair descent, prolonged sitting (where the knee is passively held in this range), and mid-depth squatting rather than at full knee flexion where the patella is more deeply seated in the trochlear groove and less susceptible to lateral displacement forces.
The Squat Depth Limitation Mechanism
Rectus femoris tightness limits squat depth through two simultaneous mechanisms. First, the hip extension limitation at the starting position requires the pelvis to tilt anteriorly to achieve the hip-neutral starting position for a barbell squat, which loads the lumbar spine into extension and restricts the available hip flexion range before the pelvis impinges. Second, during the descent, the combined hip flexion and knee flexion of the deep squat bottom position requires maximum rectus femoris length. A tight rectus femoris runs out of available length before the full depth is achieved, producing either a pelvic tuck (butt wink) as the pelvis posteriorly tilts to create additional rectus femoris length, or an early heel rise as the body reduces the combined hip-knee flexion demand by shifting weight forward.

The Thomas Test and Modified Thomas Test: Assessing Rectus Femoris Tightness
Why Assessment Precedes Intervention
Not all limited squats or anterior knee pain are caused by rectus femoris tightness. Multiple structures limit squat depth (ankle dorsiflexion, hip flexor capsular restriction, thoracic mobility), and multiple factors contribute to anterior knee pain (VMO weakness, hip abductor weakness, iliotibial band tightness, patellar alignment). Performing the Thomas test before beginning a rectus femoris intervention confirms that rectus femoris tightness is genuinely the limiting factor rather than another structure that the rectus femoris stretching will not address.
The Standard Thomas Test
Lie on the back at the edge of a plinth or table with both knees bent and both thighs held to the chest. Allow one leg to lower toward the floor, extending at the hip while maintaining the other thigh held firmly against the chest to prevent lumbar extension compensation. Observe the lowering leg.
Normal: the thigh of the lowering leg should reach approximately horizontal (parallel to the floor) and the knee should remain at approximately 90 degrees of flexion as the hip extends. Hip flexor (iliopsoas) tightness is present if the thigh cannot reach horizontal. Rectus femoris tightness is specifically present if the knee extends (straightens) as the thigh lowers — the knee must extend because the tight rectus femoris cannot simultaneously allow both hip extension and knee flexion at the same time.
The Modified Thomas Test for Isolated Rectus Femoris Assessment
The modified Thomas test isolates rectus femoris tightness more specifically. Lie on the back at the table edge. Pull both knees to the chest, then lower the tested leg while a partner applies gentle downward pressure on the lowered thigh to achieve full hip extension. Observe the knee angle of the lowered leg.
If the knee can remain at 90 degrees of flexion while the thigh is at horizontal, the rectus femoris is adequately flexible. If the knee spontaneously extends toward less than 90 degrees of flexion, the rectus femoris is tight by the degree to which the knee extends past 90 degrees. A knee angle of 70 degrees (20 degrees extension from 90) indicates moderate tightness. A knee angle of 45 degrees indicates significant tightness that is likely contributing to both squatting limitations and anterior knee pain.
The Prone Knee Bend Test
Lie face down on the floor (prone position). Have a partner passively flex the knee, bringing the heel toward the buttock. Normal rectus femoris allows full knee flexion to the heel-to-buttock range without the hip simultaneously flexing (lifting off the table). Rectus femoris tightness is present when the knee cannot achieve full flexion or when the hip automatically flexes as the knee is bent — the hip rises because the tight rectus femoris, unable to lengthen further at the knee end, pulls the hip into flexion as the only remaining way to reduce the length demand.
Correlating Assessment to Movement Patterns
Assess the Thomas test result alongside a bodyweight squat observation. If the squat assessment shows early heel rise, forward trunk lean, or limited depth, and the Thomas test shows knee extension past 80 degrees (indicating moderate-to-significant rectus femoris tightness), the rectus femoris is likely a primary limiter. If the squat shows limited depth but the Thomas test is normal, ankle dorsiflexion or hip capsular restriction is more likely the limiting factor. The ankle mobility assessment and how it interacts with squat depth limitation is covered in the ankle mobility guide.
Red Flags: When Assessment Indicates More Than Tightness
Three findings during the Thomas test assessment indicate that rectus femoris stretching alone is insufficient and that physiotherapy assessment is appropriate. First, pain at the anterior hip during the hip extension component that reproduces the patient’s symptoms — possible AIIS or hip flexor origin pathology. Second, anterior knee pain specifically reproduced during the modified Thomas test knee flexion component — possible patellar tendinopathy or PFPS that may require specific rehabilitation rather than stretching alone. Third, neurological symptoms (tingling, numbness, or shooting pain) during the prone knee bend test — possible femoral nerve involvement that requires neural mobilisation rather than muscle stretching.
Beginner Level: Foundational Rectus Femoris Stretching
Why Beginners Need Specific Rectus Femoris Stretches Rather Than Generic Quad Stretches
Standing quad stretches performed by pulling the ankle toward the buttock while standing on one leg are commonly performed as rectus femoris stretches. They produce a quad stretch, but they typically do not adequately stretch the rectus femoris’s hip origin because the standing position allows the hip to flex slightly forward as the knee flexes, reducing the tension at the proximal attachment. Effective rectus femoris stretching must simultaneously extend the hip and flex the knee to create tension at both the proximal (hip) and distal (knee) attachments of the two-joint muscle.
🔄 1. Half-Kneeling Rectus Femoris Stretch (Lunge Position)
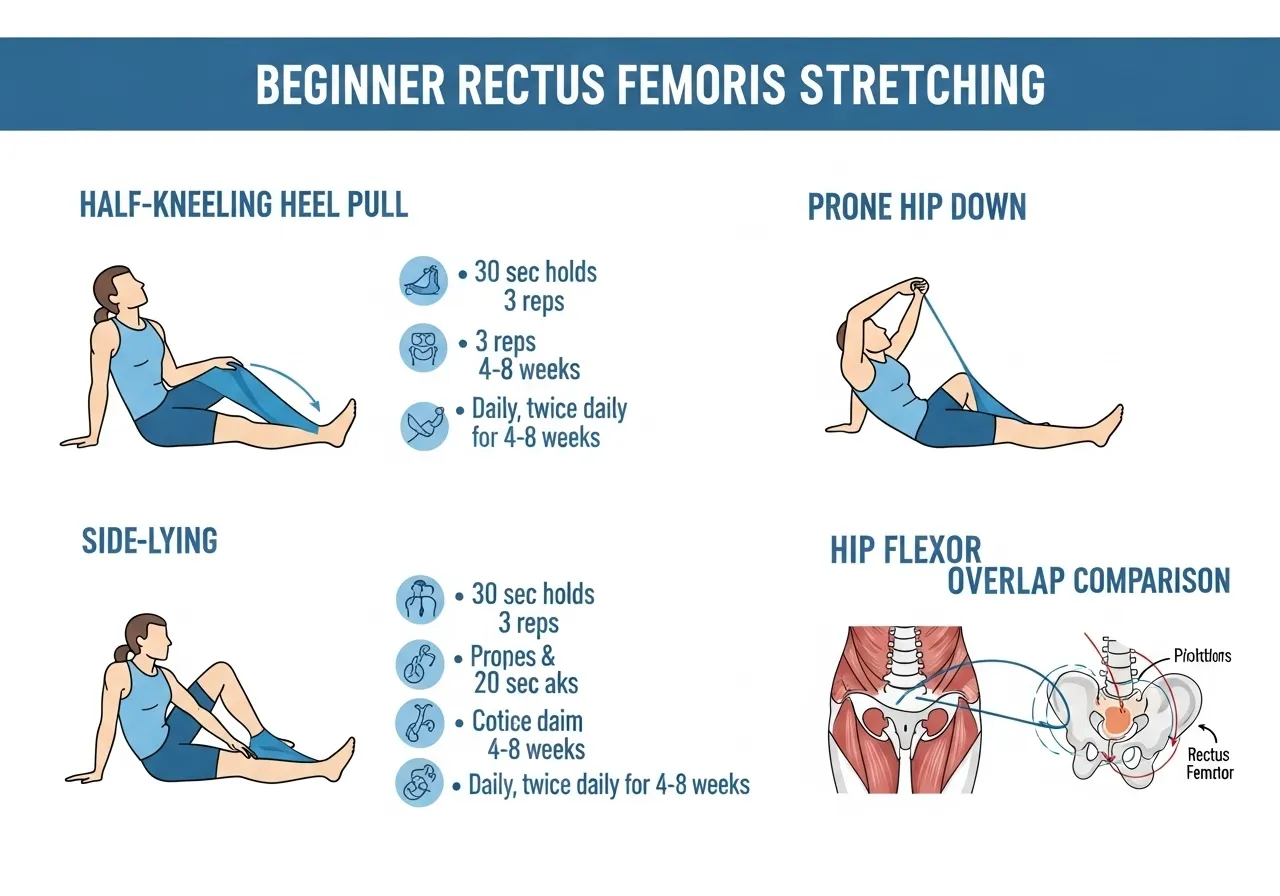
How: Kneel on one knee with the stretched-side knee down. The opposite foot is forward in a lunge position. Shift the hips forward until a stretch is felt at the front of the rear thigh, near the hip. Hold 30 seconds. Perform 3 repetitions per side.
Key point: The key difference from a standard hip flexor stretch is that the heel of the rear foot should be pulled toward the buttock by reaching back and holding it with the hand on the same side. This knee flexion component is what specifically stretches the rectus femoris rather than just the iliopsoas.
🔄 2. Prone Rectus Femoris Stretch
How: Lie face down (prone). Bend the knee of the side being stretched, reaching back to hold the ankle with the hand on the same side. Draw the heel toward the buttock while pressing the hip of the stretched side firmly into the floor. Hold 30 seconds. Perform 3 repetitions.
Key point: Pressing the hip into the floor prevents the automatic hip flexion that the tight rectus femoris induces when the knee is flexed in this position. The hip must stay down for the stretch to reach the proximal rectus femoris attachment rather than only the distal quad.
🔄 3. Side-Lying Quad and Rectus Femoris Stretch
How: Lie on the non-stretched side. Reach back with the top arm to hold the top ankle, drawing the knee toward a bent position behind the body. Allow the hip to extend naturally as the knee flexes, which stretches the rectus femoris across both joints. Hold 30 seconds. Perform 3 repetitions.
Key point: The side-lying position makes it easier to maintain hip extension (preventing the hip from flexing forward) while flexing the knee, which is the combination required for rectus femoris stretch. This variation is more comfortable for people with knee pain that limits the prone position.
Beginner Protocol and Frequency
For trainees with confirmed moderate-to-significant rectus femoris tightness from the Thomas test assessment, daily stretching is the appropriate frequency during the first 4 to 8 weeks of the restoration programme. Twice daily (morning and evening sessions of 5 to 10 minutes) produces faster length restoration than once-daily stretching because the muscle’s adaptation to shortened length from years of sitting is not overcome by once-daily maintenance stimuli. Each session: 3 stretches per variation, 30-second holds, 2 variations per session. The hip flexor tightness and its overlap with rectus femoris restriction in desk workers is covered in the hip flexor guide.
Intermediate Level: Dynamic Stretching and Movement Integration
Beyond Static Holds: Why Dynamic Rectus Femoris Work Is Needed
Static stretching develops passive rectus femoris length but does not develop the neuromuscular control that allows the improved length to be used during dynamic activities like running and squatting. An athlete who can achieve a 30-second prone rectus femoris stretch comfortably may still show the same limited squat depth and anterior hip pull during running because the central nervous system has not learned to use the available range in movement contexts. Intermediate rectus femoris training uses dynamic and movement-integrated techniques that develop both the range and the motor pattern that utilises it.
🔄 4. Walking Lunge With Overhead Reach
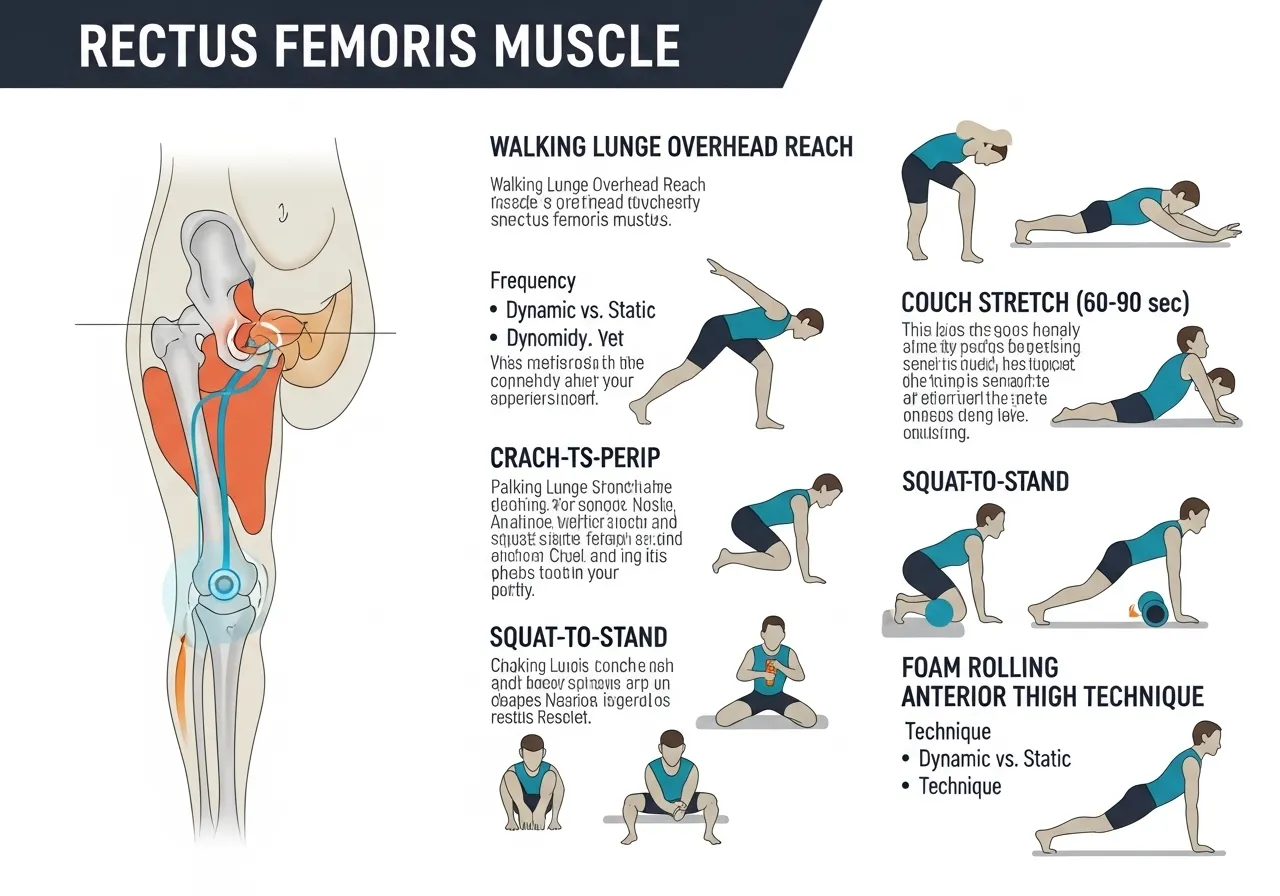
How: Perform alternating forward lunges, reaching both arms overhead as the back knee approaches the floor. The overhead reach accentuates the hip extension of the trailing leg by increasing the thoracic extension and shoulder elevation that demand greater rectus femoris lengthening. Perform 10 lunges per side continuously.
Key point: The overhead reach extends the rectus femoris stretch from a lower-body-only stretch to a full anterior chain stretch. This is the dynamic equivalent of the half-kneeling stretch and develops the rectus femoris length in the movement context that running and athletic activities demand.
🔄 5. Couch Stretch (Elevated Rear Foot Lunge Stretch)
How: Kneel with one knee on the floor and the rear foot elevated against a wall or couch behind. The knee of the rear leg is bent to approximately 90 degrees with the foot elevated. Shift the hips forward and down while maintaining an upright torso to create an intense rectus femoris stretch. Hold 60 to 90 seconds per side.
Key point: The couch stretch is the most intense static rectus femoris stretch available because it simultaneously maximises hip extension (through the forward hip shift) and knee flexion (through the elevated foot). Introduce it gradually — many trainees find it extremely uncomfortable initially, and forcing range too quickly produces pain rather than useful stretch stimulus.
🔄 6. Squat to Stand With Rectus Femoris Mobilisation
How: Begin in a deep squat position. From the squat, shift into a lunge by extending one leg backward while maintaining the other leg in the deep squat. Hold the lunge for 3 seconds, return to the squat, then lunge on the other side. Repeat 5 to 8 times per side.
Key point: This sequence develops rectus femoris length in the context of lower limb loading positions that transfer directly to improved squat depth and lunge mechanics. It also develops the neuromuscular coordination between the deep squat and the hip extension lunge that the rectus femoris restricts when tight.
Foam Rolling the Rectus Femoris
Foam rolling the anterior thigh before the stretching sequence reduces the resting tension in the rectus femoris and allows greater range to be achieved during subsequent stretching. Position the foam roller under the anterior thigh, supporting the upper body on the forearms. Roll slowly from just above the knee to just below the hip, pausing for 10 to 15 seconds on any tender points. Perform 60 to 90 seconds per thigh before the stretching sequence. Research on foam rolling preceding static stretching consistently shows that the combination produces greater acute range of motion improvement than either technique alone, making pre-stretch foam rolling a time-efficient addition to the stretching session.
Advanced Level: Loaded Stretching and Eccentric Strengthening
Why Stretching Alone Is Insufficient for Complete Rectus Femoris Restoration
Stretching restores passive length to the rectus femoris but does not develop the eccentric strength through the restored range that prevents re-tightening and protects against the anterior knee pain that rectus femoris tightness produces. The rectus femoris that tightens from prolonged sitting is typically not only short but also weak eccentrically through the lengthened range. Developing eccentric strength through the full hip extension-knee flexion range that rectus femoris stretching restores provides the neuromuscular foundation that makes the improved length durable under functional loading.
Loaded Rectus Femoris Stretching
Adding a light resistance band or ankle weight to the prone rectus femoris stretch creates loaded stretching that drives greater sarcomere lengthening than unloaded static stretching. The load creates a sustained tension at the end range that accelerates the long-term structural adaptation — sarcomere addition — that produces permanent rather than temporary length improvements. For trainees with chronically tight rectus femoris who have not responded adequately to months of unloaded stretching, loaded stretching at the end range of the prone or couch stretch position provides the additional stimulus for continued length adaptation.
Eccentric Nordic Hamstring Curl Principle Applied to Rectus Femoris
The eccentric strength principle that makes the Nordic hamstring curl effective for hamstring injury prevention has a rectus femoris equivalent: the reverse nordic or kneeling lean back. From a kneeling position, lean the torso backward as far as control allows, loading the rectus femoris eccentrically as it controls the rate of posterior lean. Return to upright by contracting the rectus femoris concentrically. This exercise develops the eccentric rectus femoris strength through the lengthened range that conventional quad exercises performed in the seated knee-extension position do not address.
📅 Advanced Rectus Femoris Programme (Weeks 7 to 12)
- Couch stretch: 3 × 90 seconds per side, daily
- Loaded prone stretch with ankle weight (0.5 to 1 kg): 3 × 60 seconds, 3 days per week
- Reverse nordic (kneeling lean back): 3 × 8 controlled reps, 3 days per week
- Split squat with controlled rear knee descent: 3 × 10 per side (loaded eccentric)
- Weekly Thomas test assessment to track progress
This programme combines maximum passive length restoration (couch stretch), structural length adaptation through load (loaded prone stretch), and eccentric strength development through the restored range (reverse nordic). All three components address the different aspects of the rectus femoris restoration that stretching alone cannot achieve.
Integrating Rectus Femoris Work Into Squat Training
As rectus femoris length improves through the stretching and strengthening programme, squatting mechanics typically improve spontaneously — the heel rise and forward trunk lean that characterised early squatting attempts diminish as the muscle’s restriction is lifted. However, the motor pattern of the compensatory squatting mechanics may persist as a habit after the physical restriction is resolved. Deliberate practice of correct squat depth with bodyweight and then light load, focusing on maintaining heel contact throughout and allowing the hips to descend vertically rather than pushing them forward, reinforces the new mechanical pattern that the improved rectus femoris length enables. The QL tightness that often co-exists with rectus femoris restriction in desk workers is covered in the QL guide.
Managing the Compensatory Patterns: Hip and Lumbar Consequences of Rectus Femoris Tightness
Anterior Pelvic Tilt: The Most Common Compensation
Anterior pelvic tilt — the pelvis tilting forward so the front of the pelvis drops and the back rises, increasing the lumbar lordosis — is the primary compensation for tight hip flexors including the rectus femoris. When the rectus femoris limits hip extension, the pelvis must tilt anteriorly to achieve the forward stride of walking, running, or the standing upright position. Over time, this compensatory anterior tilt becomes the habitual resting pelvic position that persists even after the acute rectus femoris tightening episode resolves.
Correcting anterior pelvic tilt requires addressing both the tight structures that pull the pelvis forward (rectus femoris, iliopsoas) and the weak structures that should resist the forward pull (gluteus maximus, hamstrings, lower abdominals). Releasing the rectus femoris through the stretching programme above addresses the tight side of the equation. Developing glute and hamstring strength through Romanian deadlifts, hip thrusts, and single-leg exercises addresses the weak side.
Lumbar Extension Compensation During Running
Runners with rectus femoris-limited hip extension compensate by extending the lumbar spine further during late stance to create the appearance of adequate hip extension without actual hip joint movement. Over high mileage volumes, this lumbar hyperextension creates cumulative stress at the lumbar facet joints and the posterior disc that produces the lower back pain runners often attribute to running volume rather than to the biomechanical compensation driven by hip flexor restriction.
Addressing the rectus femoris and restoring genuine hip extension range — confirmed by the Thomas test showing the thigh reaching horizontal with the knee maintaining 90 degrees of flexion — is the appropriate intervention for runners with this pattern. The lumbar pain typically resolves within 4 to 6 weeks of restored hip extension range as the lumbar extension compensation disappears from the running pattern.
Patellar Tendon Strain and Osgood-Schlatter in Adolescents
In adolescent athletes, rectus femoris tightness relative to rapid bone growth is a contributing factor to Osgood-Schlatter disease — the painful tibial tuberosity apophysitis that affects growing athletes. During growth spurts, the femur and tibia lengthen faster than the rectus femoris and patellar tendon system can adapt, creating relative tightness that places elevated tension on the tibial tuberosity apophysis during the quadriceps’ concentric contractions of jumping, running, and squatting. Rectus femoris stretching and relative reduction of high-impact loading are the primary management approaches for Osgood-Schlatter during active growth phases.
Knee Extension Lag and Late-Stage Rehabilitation
Rectus femoris shortening contributes to the knee extension lag (inability to fully extend the knee against gravity) seen in some post-surgical and post-immobilisation rehabilitation scenarios. After periods of knee immobilisation in flexion, the rectus femoris adapts to the shortened position and loses the extensibility needed to allow full knee extension. In this rehabilitation context, progressive rectus femoris stretching alongside active knee extension strengthening is the appropriate dual intervention.
The Fascia Connection: Rectus Femoris and the Anterior Chain
The rectus femoris is part of the anterior superficial myofascial line — a continuous fascial chain connecting the dorsum of the foot, through the tibialis anterior, quadriceps, rectus femoris, rectus abdominis, and sternochondral fascia to the sternocleidomastoid. Tightness at any point in this chain creates tension throughout. Desk workers with tight rectus femoris often show concurrent abdominal fascial tension, reduced thoracic extension, and forward head posture that are all manifestations of the same shortened anterior chain.
Frequently Asked Questions About Rectus Femoris Tightness
How long does it take to see improvement in squat depth from rectus femoris stretching?
Trainees with moderate rectus femoris tightness typically see measurable improvement in squat depth within 3 to 4 weeks of twice-daily targeted stretching. The early improvements reflect acute viscoelastic changes in muscle extensibility. Structural length restoration through sarcomere adaptation requires 8 to 12 weeks of consistent work. Trainees who have had significant rectus femoris tightness for years, characterised by a Thomas test knee angle well past 70 degrees (considerably less than 90), should expect the full structural restoration to take 3 to 6 months of consistent twice-daily stretching and the eccentric strengthening programme described above.
Should I stop squatting while working on rectus femoris flexibility?
Stopping squatting is generally not necessary and may be counterproductive. Squatting at the depth that the current rectus femoris length allows, without forcing range that the muscle cannot currently provide, maintains the squatting stimulus while the flexibility programme gradually extends the available range. Box squatting at a height appropriate for the current depth is a useful tool during rectus femoris restoration — the box allows the depth to be set precisely at what the muscle currently allows and progressively lowered as flexibility improves. The box squat and its relationship to movement restrictions in the squat pattern is covered in the box squat guide.
Is the couch stretch necessary, or will the simpler stretches be enough?
For mild to moderate rectus femoris tightness, the half-kneeling stretch and prone stretch with knee flexion are typically sufficient to produce complete restoration within 8 to 12 weeks of twice-daily practice. The couch stretch’s more intense combined hip extension and knee flexion demand is most valuable for trainees with significant tightness (Thomas test showing knee angle of 60 degrees or less) or for trainees who have plateaued with the simpler stretches after 6 to 8 weeks without continuing improvement. It is a progression tool rather than a baseline requirement.
Can rectus femoris tightness cause knee pain even without activity?
Yes. Prolonged sitting in the 90-degree knee flexion position places the patella in a range where rectus femoris tension creates continuous compressive force on the patellofemoral joint. Over hours of sitting, this continuous low-grade compression produces the anterior knee pain and stiffness that many desk workers experience when rising from prolonged sitting — the first few steps are painful and stiff before the joint warms up and the compressive loading becomes dynamic rather than sustained. This sitting-related anterior knee pain pattern is a hallmark of rectus femoris-driven patellofemoral compression and responds well to the stretching programme described above alongside regular movement breaks that interrupt the sustained sitting position.
How do I know if it is my rectus femoris or my hip flexors causing my squat depth limitation?
The Thomas test differentiates between rectus femoris and iliopsoas (hip flexor) tightness. If the thigh cannot reach horizontal when the other leg is held to the chest, the iliopsoas is the primary restrictor — the hip flexor crosses only the hip and limits hip extension regardless of knee angle. If the thigh reaches horizontal but the knee spontaneously extends past 90 degrees, the rectus femoris is the primary restrictor — the two-joint muscle is specifically limited when both hip extension and knee flexion are simultaneously required. Both muscles may be tight simultaneously, in which case both the hip-extension limitation and the knee-extension spontaneous movement are present, and both must be addressed for complete squat depth restoration.
- The rectus femoris crosses both the hip and knee, making it uniquely susceptible to tightening from prolonged sitting and uniquely capable of creating multi-joint restrictions when tight — limiting squat depth, hip extension in running, and contributing to anterior knee pain simultaneously.
- Rectus femoris tightness is significantly associated with PFPS. Soft-tissue tightness including rectus femoris contributes to abnormal patellar tracking and patellofemoral joint overload that standard VMO strengthening alone does not address.
- The Thomas test differentiates rectus femoris tightness (knee extends past 90 degrees as the thigh lowers) from iliopsoas tightness (thigh cannot reach horizontal). The distinction directs the specific stretching intervention correctly.
- Effective rectus femoris stretching must simultaneously extend the hip and flex the knee. Standing quad stretches that allow the hip to flex forward do not adequately stretch the rectus femoris’s proximal attachment.
- Structural restoration requires 8 to 12 weeks of twice-daily stretching. Supplement with eccentric strengthening (reverse nordic) through the restored range to develop the functional strength that prevents re-tightening and protects against knee pain recurrence.











