Hip rotation mobility is one of the most clinically significant and least directly trained movement qualities in recreational athletes. Most trainees address hip flexor tightness, hip mobility drills, and ankle dorsiflexion without ever specifically assessing or training the rotation available at the hip joint itself.
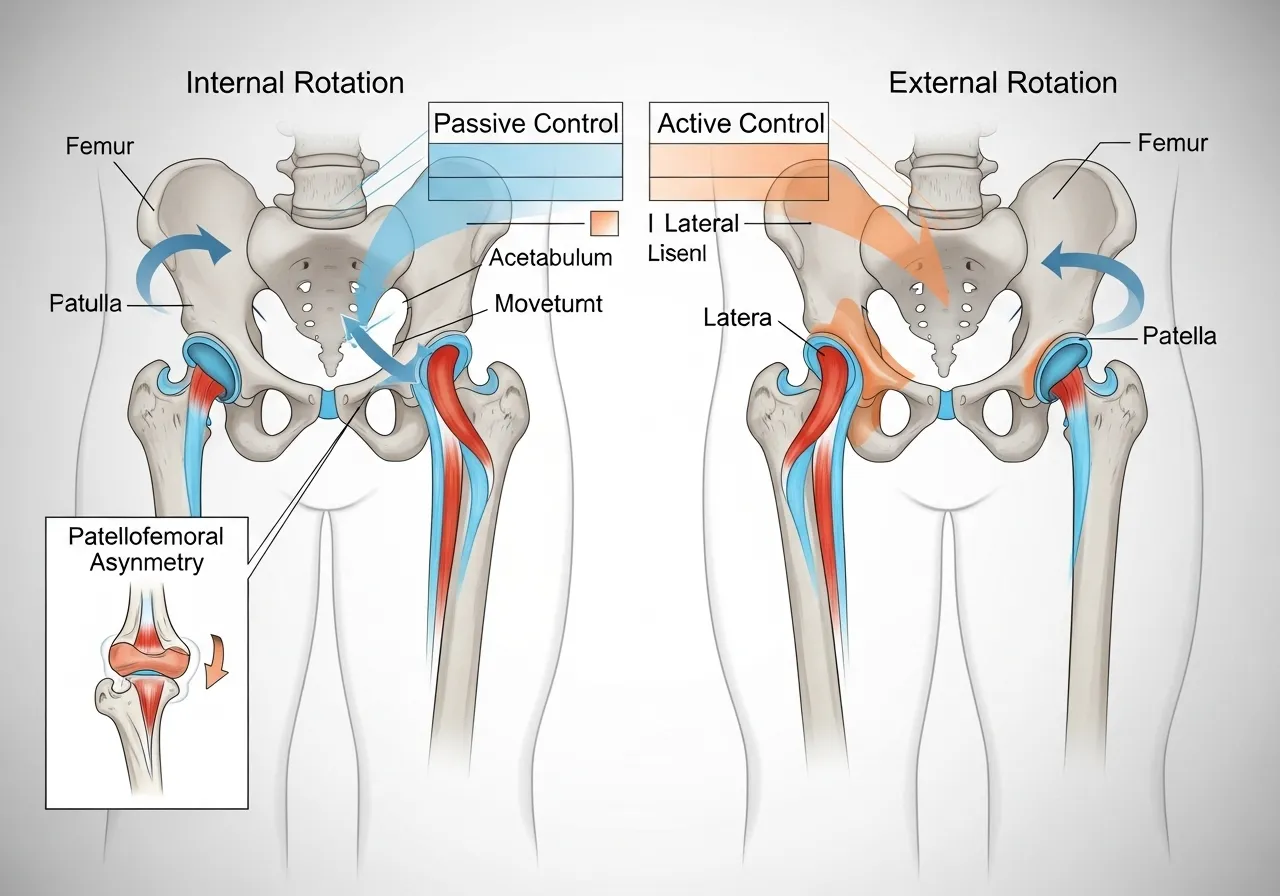
Internal and external rotation of the hip are the movements that allow the femur to rotate within the acetabulum. They are required for every squat, every running stride, every change of direction, and every rotational sport movement. When these ranges are restricted, the body compensates at the knee, lumbar spine, or ankle, creating loading patterns that produce overuse injury through movements that should be risk-free.
This guide covers what the research shows about hip rotation range, how restriction links to ACL injury risk and squat mechanics, how to assess your own restriction, and a structured mobility restoration protocol with specific exercises targeting both internal and external rotation.
Research 1: Hip Internal Rotation Restriction and ACL Injury Risk
📌 Key Finding
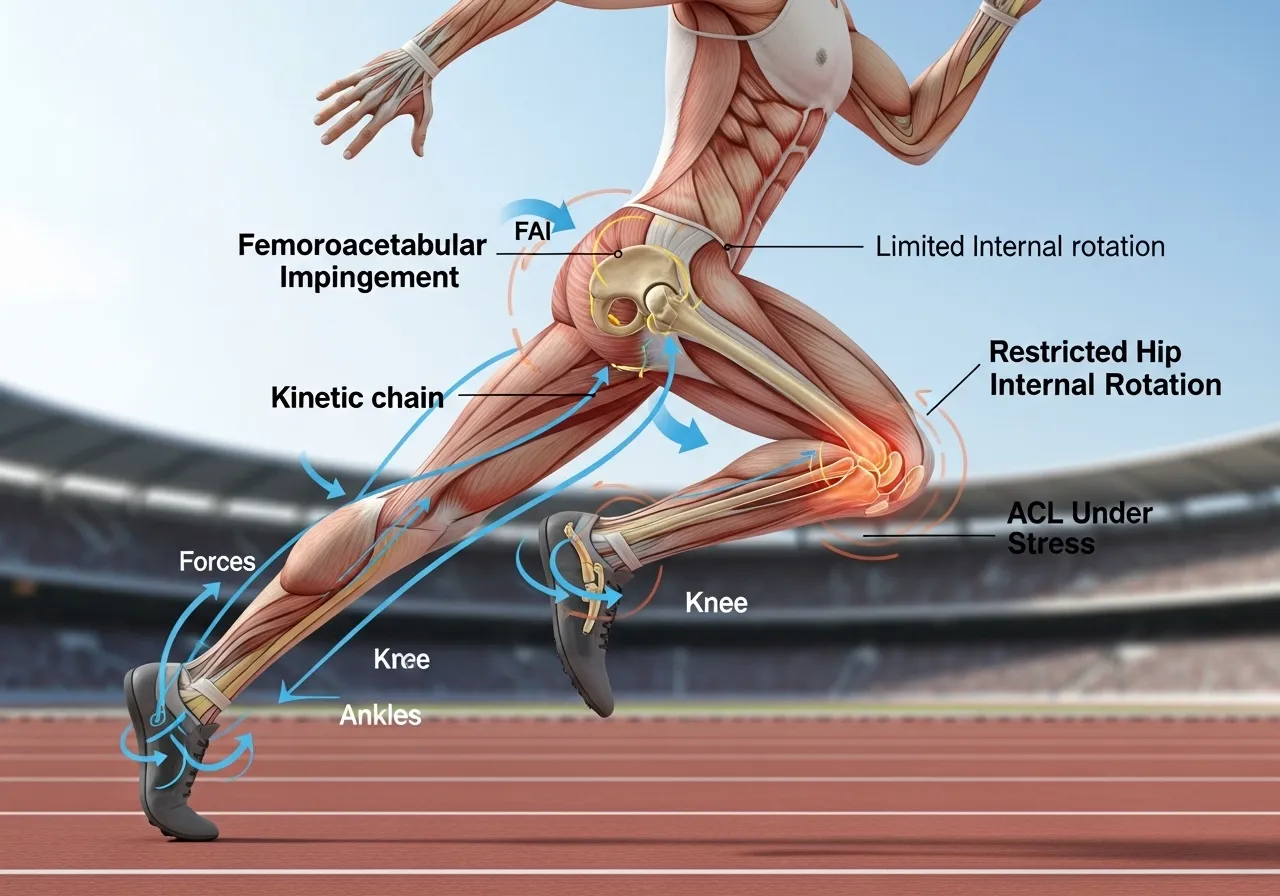
Restricted hip internal rotation in elite athletes is directly associated with increased ACL injury risk. The hip and knee operate as a kinetic chain: rotation restriction at the hip creates compensatory knee stress during the landing, cutting, and deceleration movements that most ACL injuries involve.
Why Internal Rotation Restriction Loads the ACL
When the hip lacks adequate internal rotation range, the body must find the rotation somewhere else during athletic movement. The knee, which is not a primary rotation joint, absorbs the compensatory rotation demand. During landing and cutting movements, this manifests as excessive tibial rotation and knee valgus, both of which increase ACL tensile load. The ACL injury does not originate at the knee. It originates at the hip restriction that the knee is forced to compensate for.
This mechanism explains why ACL injury prevention programmes that focus exclusively on knee mechanics (landing technique, knee valgus correction) produce incomplete protection. The proximal hip rotation restriction that generates the downstream knee stress remains unaddressed. A comprehensive approach addresses both hip rotation mobility and the neuromuscular control that converts improved mobility into functional movement patterns.
The Femoroacetabular Impingement Connection
Femoroacetabular impingement (FAI) is the most common structural cause of hip internal rotation restriction in athletes. FAI occurs when the femoral head or acetabular rim creates bony impingement at the end ranges of hip flexion combined with internal rotation. The impingement limits the available internal rotation range and produces pain or discomfort at the end of range that creates a protective neuromuscular response further restricting the movement.
FAI exists on a spectrum from mild restriction requiring mobility work to severe structural impingement requiring surgical assessment. Trainees with sharp hip pain at end-range internal rotation, clicking or catching during hip rotation movements, or persistent groin pain during squatting should obtain imaging assessment before beginning aggressive hip rotation mobility work. Mobility exercises for mild restriction are appropriate; forced rotation against structural impingement is not.
Research 2: Hip Rotation in Runners and How Range Affects Injury Pattern
📌 Key Finding
Running demands significantly greater hip internal rotation range than walking. Excessive passive hip internal rotation combined with weakness of hip external rotators is associated with patellofemoral knee pain in runners. Both range and strength must be addressed together for running-related hip and knee pathology.
The Asymmetry Problem
Hip rotation asymmetry between legs is more clinically relevant than absolute restriction in either direction. A runner with 45 degrees of internal rotation on the right and 25 degrees on the left does not have a left-hip restriction problem that can be addressed in isolation. The asymmetry creates differential loading between limbs across thousands of running strides, accumulating stress on the restricted side disproportionately to what the bilateral average would suggest.
Assessment of both legs independently, not just average range, is therefore the appropriate clinical approach for identifying hip rotation problems. A trainee with apparently adequate average rotation who has significant side-to-side differences may be at greater injury risk than one with moderate but symmetrical restriction in both directions.
The Rotation-to-Strength Ratio
Passive hip rotation range without the external rotator and internal rotator strength to control it throughout that range is not functional mobility. A hip with 50 degrees of external rotation that the gluteus maximus and external rotators cannot eccentrically control through 40 degrees is functionally less stable than a hip with 35 degrees of well-controlled external rotation. The mobility goal is not maximum range but controlled range: the range the musculature can actively manage under athletic loads.
Research 3: How Hip Rotation Position Changes Muscle Activation During Squatting
Internal and External Rotation Effects on Quad and Glute Activation
📌 Key Finding
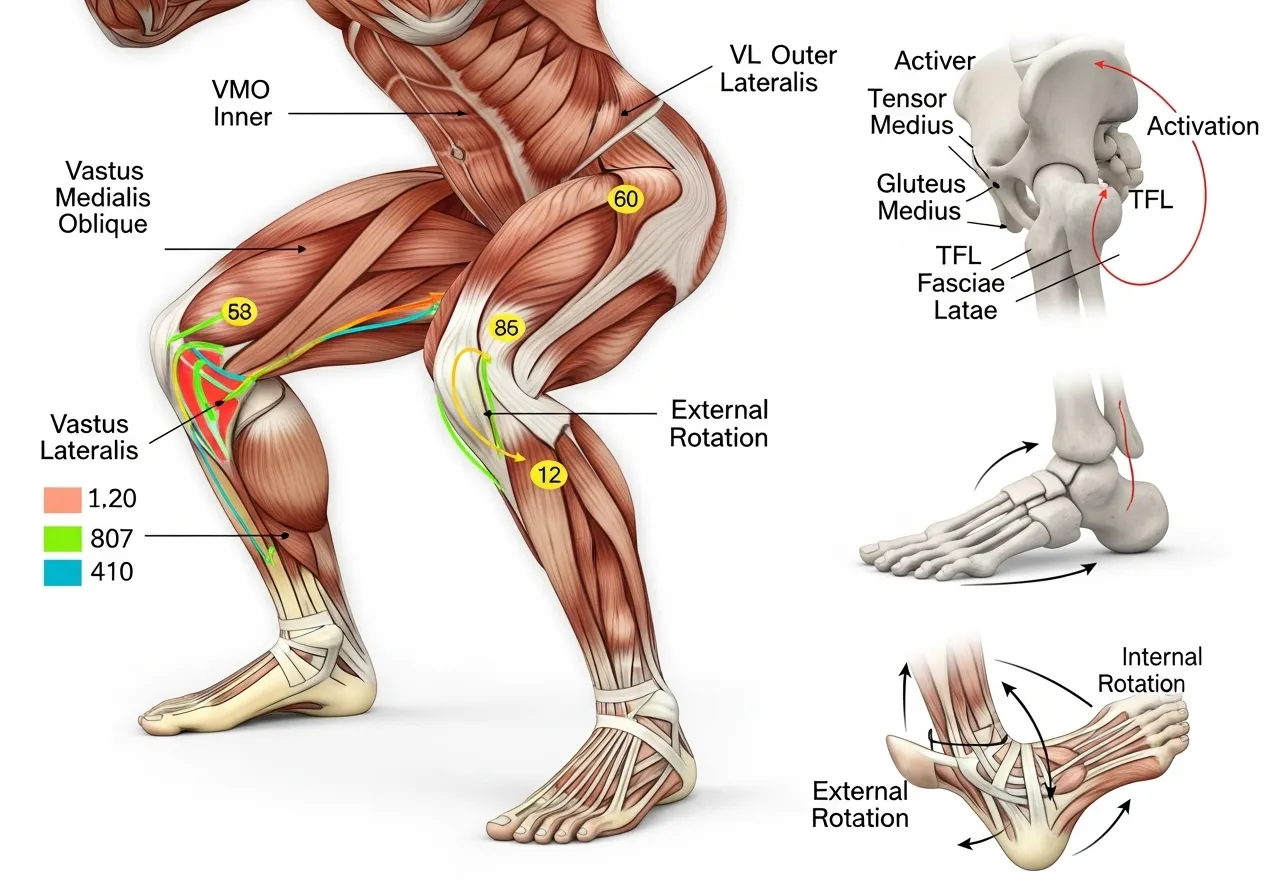
Hip rotation position during squatting measurably changes VMO-to-VL ratio and gluteus medius-to-TFL ratio. Foot and hip rotation position is not merely a comfort preference but a variable that shifts the relative demand between key muscles throughout the movement.
What This Means for Squat Foot Position
The foot angle chosen for squatting reflects available hip external rotation range. A trainee who squats with feet turned significantly outward (30 to 45 degrees) is using external rotation to compensate for limited internal rotation availability. This toe-out position allows adequate squat depth but places the hip in a biased external rotation throughout the movement, loading the TFL disproportionately and potentially underloading the gluteus medius at specific phases of the lift.
Improving internal rotation range does not require changing foot position immediately. It allows the option of varying foot position to address different muscle emphases and to reduce the accumulation of TFL overuse that constant extreme toe-out squatting can produce over years of training. The back squat depth, bar position, and how foot angle affects the muscle activation profile is covered in detail in the barbell back squat guide.
How Do You Know If Your Hip Rotation Is Actually Restricted?
The Seated Hip Rotation Test
The most accessible self-assessment for hip rotation range uses a seated position that controls pelvic compensation. Sit on a flat surface with hips and knees at 90 degrees. Keep the thigh fixed against the surface throughout the test. For internal rotation: allow the foot to swing outward while the thigh stays fixed. For external rotation: allow the foot to swing inward. Observe how far the foot moves before the pelvis begins to tilt or the thigh lifts from the surface.
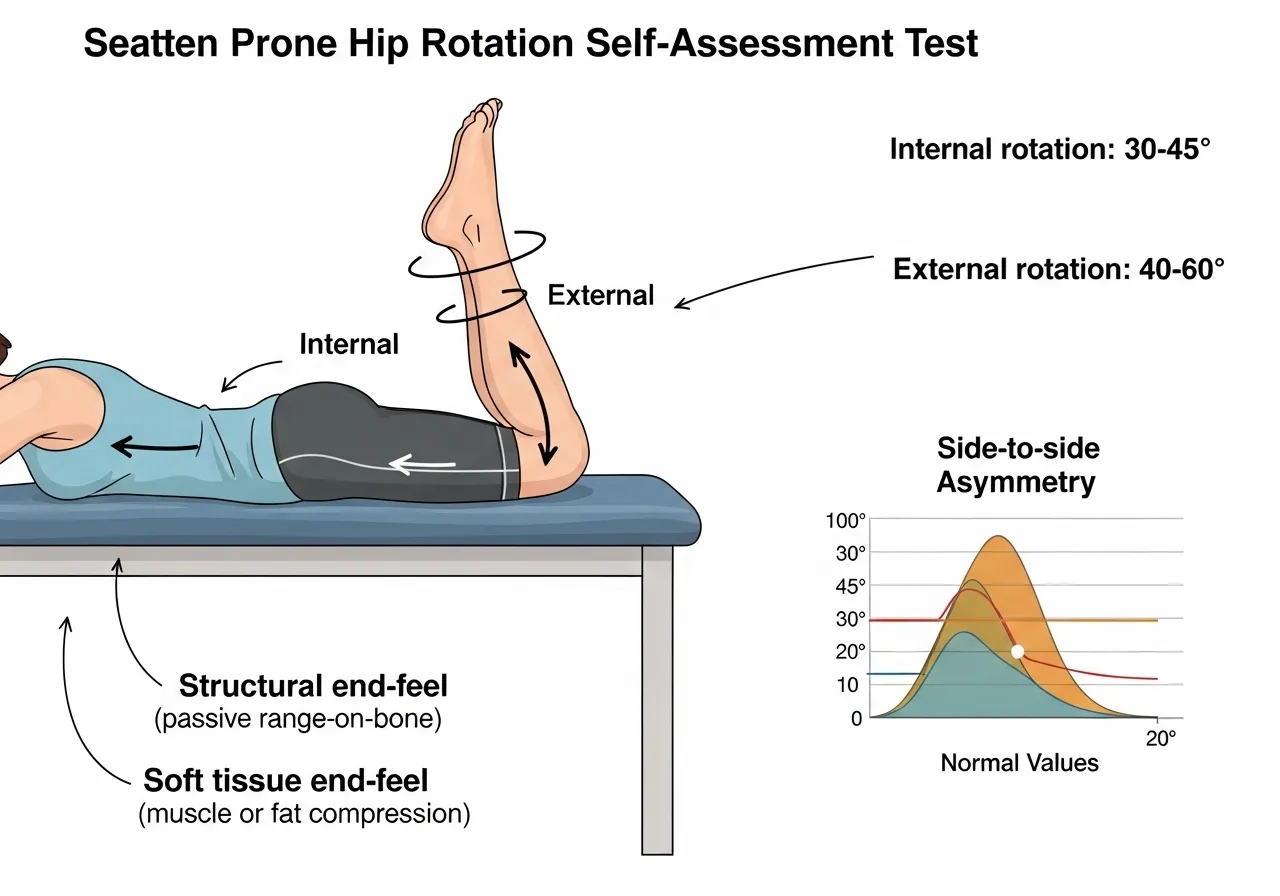
Normal internal rotation in seated position: 30 to 45 degrees. Normal external rotation in seated position: 40 to 60 degrees. A side-to-side difference of more than 10 degrees in either direction warrants deliberate mobility work on the restricted side. Measure both sides before starting any protocol to establish the asymmetry baseline that guides subsequent programming.
The Prone Hip Rotation Test
The prone position assesses hip rotation at 0 degrees of hip flexion, which reflects the range available during standing and walking mechanics rather than seated or squatting position. Lie face down with knees bent to 90 degrees. Allow both feet to fall outward together for internal rotation, or inward together for external rotation. The angle the lower leg makes from vertical approximates the rotation available.
Normal prone internal rotation: 35 to 45 degrees. Normal prone external rotation: 45 to 60 degrees. The prone test and the seated test often reveal different restriction patterns because the hip capsule and surrounding musculature are differently tensioned in each position. Both tests together provide a more complete picture of where the restriction exists than either alone.
Identifying Structural vs Soft Tissue Restriction
The end-feel at the limit of rotation distinguishes soft tissue restriction from structural restriction. A gradual, springy end-feel that responds to gentle overpressure suggests soft tissue restriction that mobility work can address. A hard, abrupt end-feel with no give suggests bony impingement or structural limitation that requires imaging assessment before aggressive mobility loading. Sharp hip or groin pain at end-range rotation, rather than a stretching sensation, is a clear signal to seek assessment rather than continuing to push the range.
The 6 Most Effective Hip Rotation Mobility Exercises
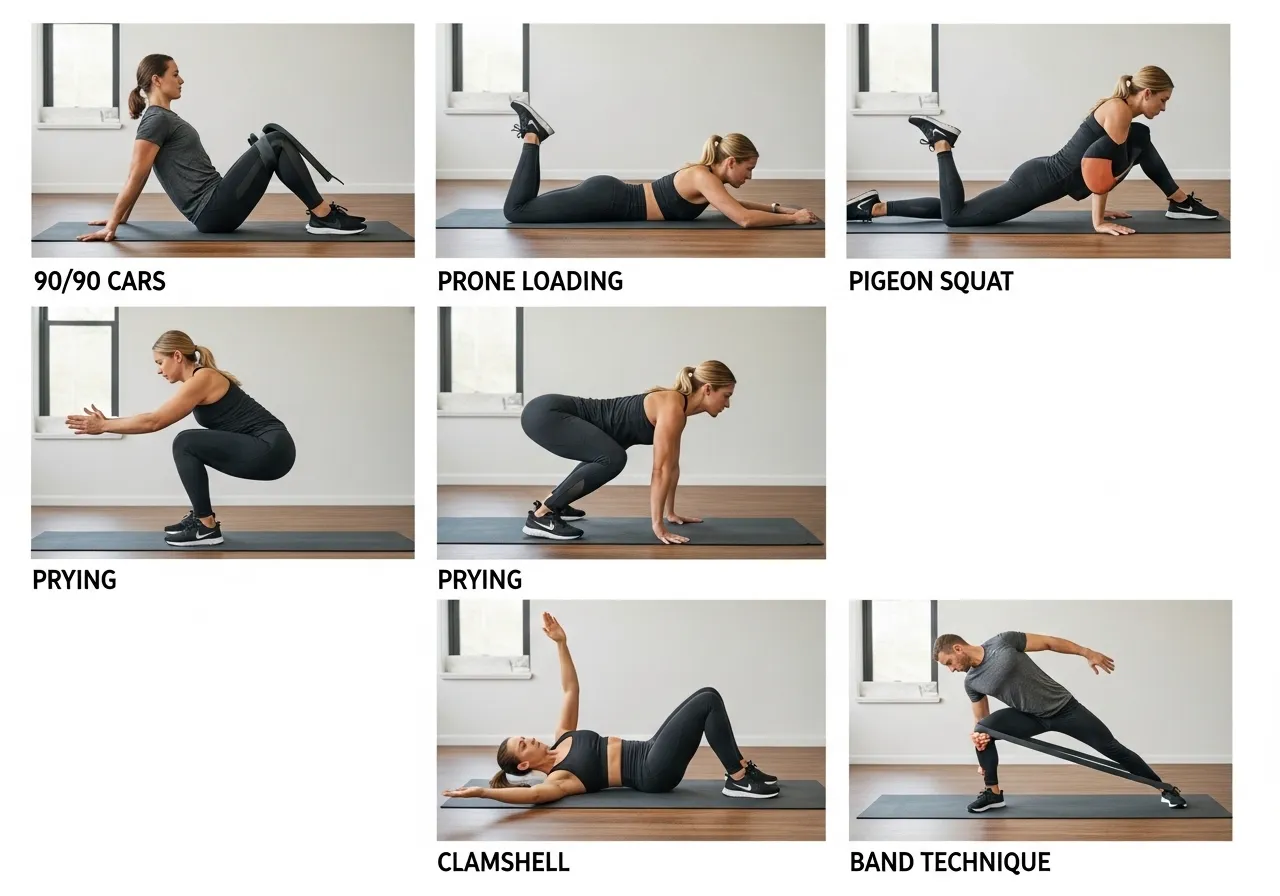
🦵 1. 90/90 Hip Rotation Stretch
Target: Both internal and external rotation from a controlled hip-flexed position
How: Sit with both hips bent to 90 degrees, one leg in front and one to the side, shins parallel. Rotate the torso toward the front leg for front hip internal rotation work. Rotate toward the rear leg for rear hip external rotation. Hold each position 30 to 45 seconds. Perform on both sides.
Key point: The 90/90 position is the foundation hip rotation mobility drill because it provides a stable base for both internal and external rotation work simultaneously. Begin here before any of the more demanding variations.
🦵 2. Hip Internal Rotation CARs (Controlled Articular Rotations)
Target: Active internal rotation range under muscular control
How: Stand on one leg. Drive the opposite knee up to hip height. From this position, rotate the raised thigh inward (internal rotation) as far as possible under active muscular control. Return. Perform 5 to 8 slow repetitions on each side.
Key point: CARs develop active control through the rotation range rather than passive flexibility. The ability to actively rotate the hip under load is more functionally relevant than passive rotation achieved through gravity or manual pressure.
🦵 3. Prone Hip Internal Rotation Loading
Target: Hip internal rotation at neutral hip flexion, external rotator eccentric lengthening
How: Lie prone with knees bent to 90 degrees. Allow both feet to fall outward simultaneously (internal rotation) under gravity. Then actively return to neutral by driving the feet back upward. Add a resistance band at the ankle for progressive loading. Hold 3 to 5 seconds at the end range before returning.
Key point: This exercise specifically develops internal rotation in the prone position that the prone assessment tests. It is the most direct training analogue to the prone assessment and produces the most specific adaptation to that tested range.
🦵 4. Seated Hip External Rotation Stretch (Pigeon Pose Variation)
Target: Hip external rotation, posterior hip capsule, piriformis
How: From a seated position, cross one ankle over the opposite knee, creating a figure-4 shape. Keeping the spine tall, lean the torso forward over the crossed leg until a stretch is felt in the glute and posterior hip. Hold 45 to 60 seconds. This is a supported, more accessible version of the yoga pigeon pose.
Key point: External rotation restriction is often secondary to piriformis and deep external rotator tightness rather than structural impingement. This stretch directly targets the posterior hip soft tissue that limits external rotation range.
🦵 5. Hip Rotation in Squat (Adductor Prying)
Target: Internal rotation in the deep hip-flexed position specific to squatting
How: Drop into a deep bodyweight squat with feet moderately wide. Place elbows on the inner knees. Alternately push one knee outward with the elbow while the other knee drops inward, creating a rocking motion that explores rotation range in the deep squat position. Spend 60 to 90 seconds.
Key point: This drill develops hip rotation range specifically in the bottom squat position where the restriction matters most. It is the most functionally specific drill for trainees whose primary complaint is limited squat depth or discomfort at the bottom of squatting.
🦵 6. Hip External Rotation Strengthening (Clamshell with Band)
Target: Gluteus medius, deep external rotators, active rotation control
How: Lie on the side with hips and knees at 45 degrees, resistance band above the knees. Keeping the feet together, rotate the top knee upward toward the ceiling against the band. Return under control. Perform 15 to 20 reps per side. The clamshell develops active external rotation strength alongside passive rotation range.
Key point: Mobility without strength is passive flexibility. The clamshell converts external rotation range into active control, developing the gluteus medius strength that stabilises the hip in external rotation during squatting and running. This exercise is the standard companion to all passive hip external rotation stretching.
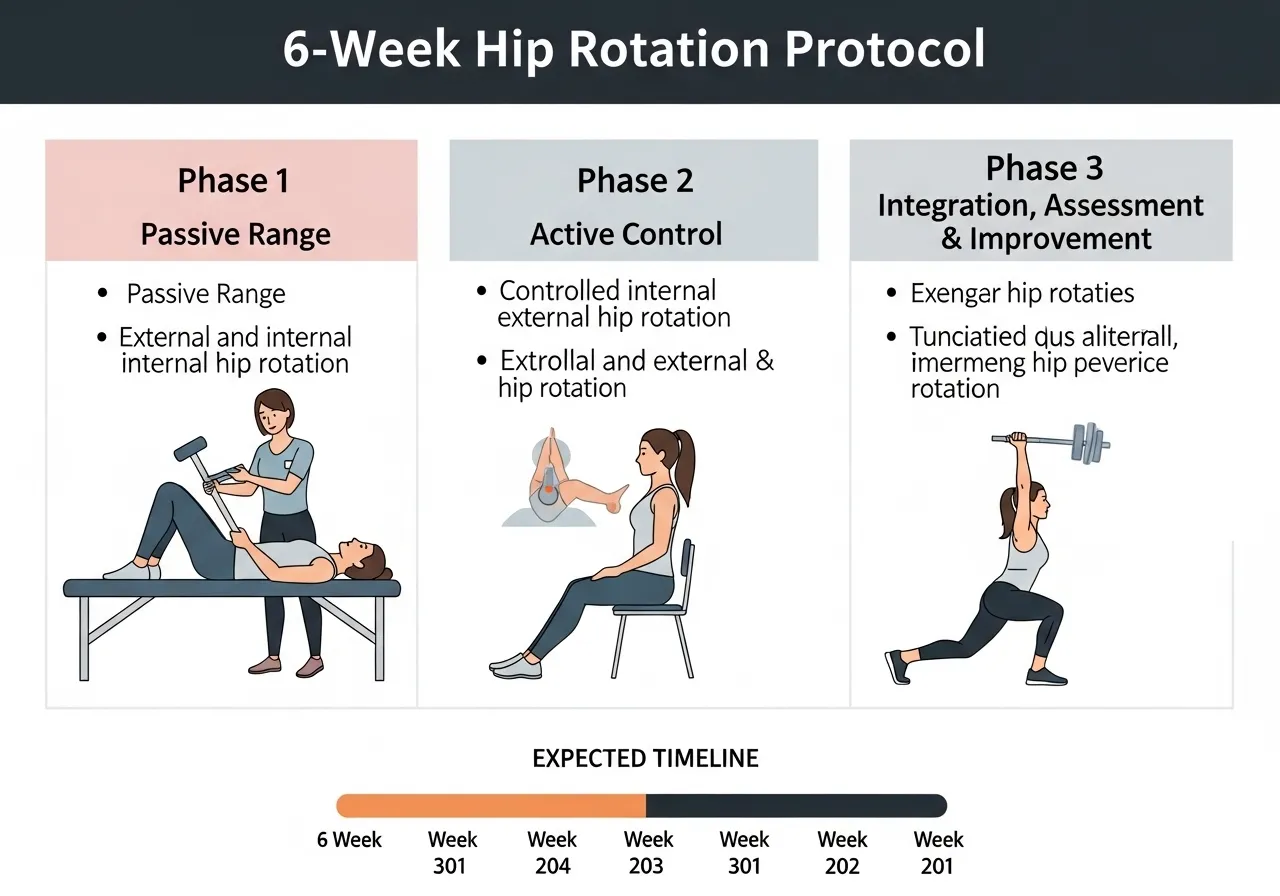
6-Week Hip Rotation Mobility Restoration Protocol
📅 Phase 1: Weeks 1 to 2: Assessment and Passive Range Development
Perform both seated and prone assessment tests to establish baseline and identify restricted direction
90/90 hip rotation stretch: 3 sets of 45 seconds each position, daily
Seated figure-4 external rotation stretch: 3 sets of 60 seconds per side, daily
Adductor prying squat: 2 minutes daily
No loaded rotation work yet. Develop passive range first
Focus: Identify which direction and which side drives the primary restriction. Most trainees find internal rotation is more restricted than external, and one side is meaningfully worse than the other. These findings direct Phase 2 emphasis.
📅 Phase 2: Weeks 3 to 4: Active Control Development
Continue passive stretches from Phase 1 (reduce to once daily)
Hip internal rotation CARs: 8 reps per side, before every training session
Prone internal rotation loading with band: 3 sets of 8 reps per side, 3 days per week
Clamshell with band: 3 sets of 15 reps per side, 3 days per week
Add extra sets on the more restricted side
Focus: Convert passive range into active control. The CARs before training sessions integrate the improved rotation range into neural patterns that transfer to loaded movement rather than only performing in isolated stretching context.
📅 Phase 3: Weeks 5 to 6: Integration and Reassessment
Maintenance stretching: 90/90 and figure-4, once daily
Continue CARs and loaded rotation work from Phase 2
Integrate rotation awareness into squatting: perform 2 sets of goblet squats focusing on driving knees out while feeling for internal rotation at the hip
Week 6: repeat assessment tests and compare to baseline
Expected: 8 to 15 degree improvement in the restricted direction
Focus: Transfer the isolated rotation gains into functional loaded movement. The goblet squat integration ensures the hip rotation range developed in isolation begins contributing to actual training movement quality. The complete hip mobility framework including deeper hip-specific drills is in the hip mobility guide.
Why Hip Rotation Restriction Returns After Treatment
The Load Pattern Problem
Hip rotation restriction in most athletes is not a stretching deficit. It is an adaptation to the load patterns the body repeatedly experiences. A runner who logs 50 km per week with consistent hip adduction and external rotation bias develops progressive tightening of the posterior hip capsule and external rotators as an adaptation to that specific load pattern. Stretching during cooldown partially offsets this adaptation. It does not reverse the underlying pattern that creates the adaptation.
Lasting improvement requires both addressing the tissue restriction and modifying the load pattern that drives the adaptation. For runners, this means gait assessment and correction of hip adduction mechanics alongside mobility work. For strength athletes, this means addressing foot and hip position during squatting and deadlifting alongside isolated rotation mobility work. The mobility restoration protocol addresses the tissue. The movement pattern correction ensures the tissue does not re-adapt to the same restriction within weeks of treatment.
Sleep and Sustained Position Effects
Hip rotation range is significantly influenced by sustained sleep positions. Side sleepers who consistently sleep with the top hip in flexion and internal rotation, effectively in a foetal position, shorten the posterior capsule and external rotators during the 6 to 8 hours the body is in that position nightly. The stretching session performed for 10 minutes before training cannot fully counteract 7 hours of the opposite position.
Placing a pillow between the knees during side sleeping maintains a more neutral hip rotation position and reduces the accumulated overnight shortening that side sleeping without support creates. This simple positioning change often produces faster improvement in hip rotation than equivalent additional stretching time, because it reduces the nightly restriction accumulation that stretching is working against.
The Strength Deficit Component
When the hip rotator muscles are weak, the joint develops protective tone as a substitute for active muscular control. The nervous system restricts passive range as a protective mechanism when it detects that the muscles cannot adequately control the joint through a wider range. This protective tightening cannot be removed by stretching because it is not structural. It resolves when the rotator muscles become adequately strong to control the available range. The clamshell progression, hip external rotation loaded carries, and single-leg squatting that develops rotator strength through functional range addresses the strength deficit that underlies protective tightening.
Frequently Asked Questions About Hip Rotation Mobility
How much hip internal rotation is normal?
Normative values for hip internal rotation vary by position and population. In seated position at 90 degrees of hip flexion, 30 to 45 degrees of internal rotation is considered normal for adults. In prone position (0 degrees of hip flexion), 35 to 45 degrees is normal. Values below 25 degrees in either position represent meaningful restriction worth addressing in active individuals.
Athletes in rotational sports (baseball, tennis, golf) often develop direction-specific asymmetries through sport-specific adaptation. A baseball pitcher typically shows reduced internal rotation in the throwing-side hip and increased external rotation as a sport-adapted pattern. These asymmetries are not pathological per se but should be monitored because extreme side-to-side differences exceed the compensation capacity of the kinetic chain and increase injury risk even when the adapted range is within normal absolute values for each direction separately.
Does hip rotation restriction cause back pain?
Restricted hip rotation, particularly internal rotation restriction, produces compensatory lumbar rotation during movements that require hip rotation. Every step in walking involves hip internal rotation of the stance leg. When this rotation is unavailable at the hip, the lumbar spine rotates to compensate. Over thousands of steps daily, this compensatory lumbar rotation accumulates rotational stress on the intervertebral discs and facet joints that contributes to mechanical lower back pain.
Many individuals with chronic non-specific lower back pain show significant hip rotation restriction on assessment. Addressing the hip rotation restriction often produces meaningful back pain reduction without any direct lumbar treatment, confirming the kinetic chain relationship between hip rotation availability and lumbar spinal loading. The ankle mobility contribution to this chain of compensations upstream to the lumbar spine is covered in the ankle mobility guide.
How long does it take to improve hip rotation range?
Initial improvements in passive hip rotation range from consistent daily stretching appear within two to three weeks. The 90/90 stretch performed daily for two weeks produces measurable increases in rotation range in most individuals without structural hip pathology. These early gains reflect primarily neurological changes, reduced protective tone and improved stretch tolerance, rather than structural tissue changes.
Structural changes, actual lengthening of the posterior hip capsule and external rotator muscle-tendon units, require four to eight weeks of consistent work. The six-week protocol above addresses both the neurological and structural components through a combination of passive stretching, active CARs, and loaded rotation exercises. Trainees with more chronic restriction often require 8 to 12 weeks before functional movement qualities, specifically squat depth and single-leg balance, reflect the range improvements measured in isolated assessment positions.
Key Takeaways
Restricted hip internal rotation is directly associated with increased ACL injury risk in elite athletes through the kinetic chain mechanism that transfers hip restriction into compensatory knee stress during cutting and landing movements.
Running demands significantly greater hip internal rotation than walking. Excessive passive internal rotation combined with hip external rotator weakness underlies patellofemoral pain in many runners.
Hip rotation position during squatting changes VMO-to-VL ratio and gluteus medius-to-TFL ratio. Foot angle preference reflects available hip rotation range, not optimal muscle recruitment.
Assess both seated and prone rotation bilaterally before starting any protocol. Side-to-side asymmetry of more than 10 degrees is more clinically significant than absolute restriction in both directions equally.
Mobility without strength is passive flexibility. Active CARs and clamshell strengthening must accompany passive stretching to convert range into functional control that transfers to loaded movement.
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only and does not replace professional medical or fitness advice.If you have chronic lower back pain, spinal pathology, or any musculoskeletal condition — please consult a qualified physiotherapist or healthcare professional before beginning any core stability program. Core stability training has evolved…
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only. It does not replace professional medical or fitness advice. If you have any pre-existing condition, injury, or health concern — consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program. Hip flexor tightness is one…
⚠️ Wrist Safety NoteWrist mobility exercises involving loaded extension or flexion place stress on the distal radius, carpal bones, and triangular fibrocartilage complex (TFCC). Individuals with active wrist tendinopathy, carpal tunnel syndrome, Kienbock’s disease, or a history of distal radius fracture within 12 months should obtain physiotherapy clearance before starting progressive wrist loading. Sharp or…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. ⚠️ Medical Disclaimer: This article is for general informational purposes only…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only. It does not replace professional medical advice. If you have existing shoulder pain, rotator cuff injury, or shoulder impingement, consult a qualified healthcare professional before starting any scapular training programme. Most shoulder problems in the gym do not start at the shoulder joint…
Shoulder internal rotation is one of the most commonly restricted ranges of motion in both overhead athletes and office workers, for completely different reasons that produce the same mechanical consequence: the humeral head cannot sit centrally in the glenoid during overhead movements, the supraspinatus tendon gets compressed, and pain or injury follows. In overhead athletes…