⚠️ Health & Fitness Disclaimer This article is for general educational and informational purposes only. It does not replace professional medical or fitness advice. If you have any pre-existing condition, injury, or health concern — consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program.
VO2 max is one of the most referenced metrics in endurance sports and health research — yet for most recreational exercisers, what it actually means, why it matters beyond athletic performance, and how to train it effectively remains unclear.
This guide explains VO2 max in accessible physiological terms, reviews the evidence on which training methods improve it most effectively, and provides practical programming guidance for different fitness levels.
What Is VO2 Max and Why Does It Matter for Both Health and Performance?
The Definition
VO2 max (also written V̇O₂max) is the maximum rate at which the body can consume oxygen during intense exercise, expressed in milliliters of oxygen per kilogram of body weight per minute (ml/kg/min).
During maximal effort, oxygen travels from the lungs into the bloodstream, is carried to working muscles, and is used by mitochondria (the cellular energy-producing structures) to convert fuel into ATP (adenosine triphosphate — the primary cellular energy currency). VO2 max represents the ceiling of this entire oxygen delivery and utilization system.
Why VO2 Max Matters Beyond Athletics
VO2 max is not only an athletic performance metric — it is one of the strongest independent predictors of cardiovascular health and longevity in the research literature:
📊 Higher VO2 max is consistently associated with significantly reduced risk of cardiovascular disease, type 2 diabetes, and all-cause mortality across large population cohort studies
📊 VO2 max declines approximately 10% per decade from age 25 in sedentary individuals — and approximately 5% per decade in those who maintain regular aerobic training
📊 Cardiorespiratory fitness (closely correlated with VO2 max) is sometimes described as the most powerful modifiable predictor of long-term health outcomes available in exercise science
VO2 Max Reference Ranges
Classification
Men (ml/kg/min)
Women (ml/kg/min)
Poor
<35
<28
Below average
35–41
28–33
Average
42–50
34–40
Good
51–58
41–48
Excellent
59–65
49–55
Elite endurance athlete
70–85+
60–75+
These are general population estimates that vary by age, testing protocol, and measurement method. Individual values may differ based on genetics, training history, and health status. A sports medicine physician or exercise physiologist can provide accurate testing and context-specific interpretation of results.
Genetics vs. Training: How Much of VO2 Max Is Trainable?
Research estimates that 40–60% of the variation in VO2 max between individuals is genetically determined — explaining why some people respond dramatically to aerobic training while others see modest improvements from the same training stimulus.
However, the trainable component (40–60%) is substantial. Most previously sedentary or recreationally active individuals can improve VO2 max by 15–25% with consistent aerobic training over 3–6 months. Some individuals — called “high responders” — may see 40–50% or greater improvements from the same training program.
VO2 Max and Practical Everyday Performance
Beyond the statistics on disease risk reduction and mortality, VO2 max has concrete implications for daily functional capacity that most people relate to intuitively:
Climbing stairs without becoming noticeably breathless
Sustaining physical effort (carrying heavy bags, moving furniture, active play with children) without excessive fatigue
Recovering quickly after brief periods of exertion — heart rate returning to normal within minutes
Maintaining energy levels throughout the day without a mid-afternoon energy crash driven by cardiovascular inefficiency
These daily functional markers are driven by the same underlying cardiorespiratory fitness that VO2 max quantifies — which is why improving VO2 max through regular aerobic training improves quality of daily life in observable, concrete ways beyond athletic performance metrics.
Body Weight and VO2 Max: The Relative vs. Absolute Distinction
VO2 max is expressed as a relative value — ml of oxygen per kilogram of body weight per minute (ml/kg/min). This means that two people with identical absolute oxygen consumption capacity will have different VO2 max values if their body weights differ.
This has a practical implication: reducing excess body fat while maintaining aerobic fitness improves relative VO2 max — sometimes significantly. A person who loses 10 kg while maintaining the same cardiovascular training will see their measured VO2 max increase even if no change occurs in the actual capacity of their heart and muscles to use oxygen.
This does not diminish the importance of training-driven improvements — it simply means that body composition and aerobic training interact in determining measured VO2 max values.
VO2 Max Testing: What to Expect in a Lab Setting
For those interested in precise baseline measurement and ongoing tracking, laboratory VO2 max testing provides the most accurate data:
Standard maximal exercise test protocol:
1. Resting measurements (heart rate, blood pressure)
2. Progressive exercise on treadmill or cycle ergometer — workload increases every 2–3 minutes
3. Expired gas analysis throughout — measures oxygen consumed and CO2 produced
4. Test ends when subject reaches voluntary exhaustion or specific physiological criteria are met
5. VO2 max is the highest measured oxygen consumption achieved
Testing is available at university exercise physiology laboratories, sports medicine clinics, and performance centers. The test typically takes 20–30 minutes plus preparation time. Cost varies significantly by facility — from around $100–$300 at research facilities to higher prices at commercial performance centers.
Understanding the VO2 Max Decline With Age — and Why It Matters
The approximately 10% per decade decline in VO2 max in sedentary individuals is one of the most well-documented physiological aging patterns in exercise science. At this rate, a sedentary 60-year-old may have 35–40% less cardiorespiratory capacity than their 25-year-old self — with significant functional consequences for stamina, recovery from exertion, and resilience against cardiovascular disease.
The trained individual, by contrast, may retain 60–70% or more of their peak cardiorespiratory capacity at the same age — a difference that translates directly to functional independence, quality of daily life, and reduced healthcare burden in later life.
This is perhaps the most compelling practical argument for consistently maintaining aerobic training throughout adulthood: the primary benefit is not peak athletic performance but the preservation of functional cardiovascular capacity that determines quality of life decades later.
The Physiology of VO2 Max: What Aerobic Training Actually Changes
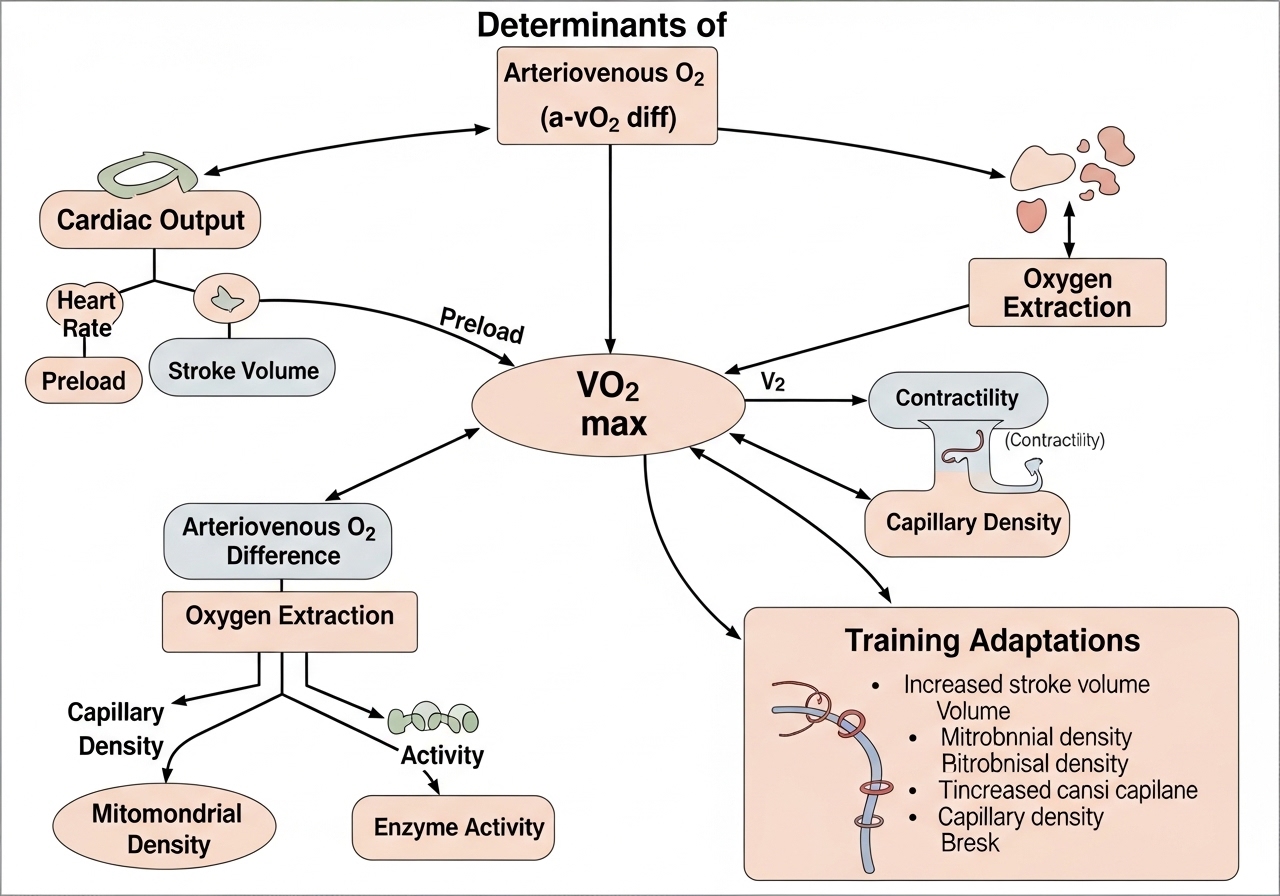
The Cardiac Output Component
The most important single determinant of VO2 max is maximum cardiac output (the volume of blood the heart pumps per minute at maximal effort), which equals:
Cardiac Output = Heart Rate × Stroke Volume (amount of blood pumped per heartbeat)
Aerobic training increases stroke volume through two mechanisms: the heart muscle itself becomes stronger and more efficient at filling and emptying, and the left ventricle (the main pumping chamber) enlarges slightly — a beneficial adaptation called cardiac hypertrophy.
This explains why endurance athletes have notably lower resting heart rates (45–55 bpm) compared to untrained individuals (60–80 bpm) — the same resting cardiac output is maintained at a lower frequency because each beat delivers more blood.
The Oxygen Extraction Component
Beyond cardiac output, VO2 max is also determined by how effectively muscles extract and use the oxygen delivered by the blood — measured as the arterio-venous oxygen difference (a-vO₂ diff).
Training adaptations that improve this peripheral component include:
Increased mitochondrial density and size in trained muscle fibers — more “engines” for aerobic energy production
Greater capillary density in trained muscles — more blood vessels delivering oxygen per unit of muscle tissue
Increased myoglobin concentration (the oxygen-storing protein in muscle fibers) in slow-twitch fibers
Enhanced fat oxidation capacity — trained muscles use fat more efficiently at submaximal intensities, sparing carbohydrate for higher-intensity efforts
The Science of VO2 Max Training: What Research Consistently Shows
Several principles emerge consistently across the VO2 max training research literature:
Intensity matters: Training must reach Zone 4 (80–90% MHR) or above to maximally stimulate VO2 max improvements — Zone 2 work alone produces peripheral adaptations but sub-maximal central cardiac stimulus
Volume matters for Zone 2: The cardiovascular benefits of Zone 2 accumulate with total weekly volume — 150–200+ minutes per week is a commonly cited target for meaningful aerobic base development
Consistency over intensity: A person who performs two HIIT sessions and one Zone 2 session per week for 12 weeks consistently will produce greater VO2 max improvements than a person who performs intensive training for 3 weeks, stops for a week, and cycles in and out
Individual response variation: Some people (“high responders”) see dramatic improvements from training; others (“low responders”) see much smaller gains from the same program. This genetic variation is well-documented and should be factored into expectations rather than attributed to training failure
VO2 Max and Different Sports: Why Values Differ
VO2 max values vary dramatically across different sports — not because some sports produce “better fitness” but because different activities recruit different muscle masses and place different demands on the cardiovascular system:
Sport / Population
Typical Elite VO2 Max (Men)
Cross-country skiing
80–96 ml/kg/min
Distance running
70–85 ml/kg/min
Cycling (road)
70–80 ml/kg/min
Swimming
60–70 ml/kg/min
Team sports (soccer, basketball)
55–70 ml/kg/min
Powerlifters / strength athletes
35–50 ml/kg/min
These ranges illustrate that elite cardiorespiratory fitness in one sport does not automatically translate to others — a world-class powerlifter may have below-average VO2 max by endurance running standards, reflecting the different physiological demands of their sport.
The Two Primary Training Methods for Improving VO2 Max
Method 1: High-Intensity Interval Training (HIIT)
HIIT involves alternating periods of near-maximal effort with recovery periods. It is generally the most time-efficient method for improving VO2 max because it specifically trains the cardiovascular system at intensities at or above VO2 max — producing strong central (cardiac) and peripheral (muscular) adaptations in less total training time.
Classic VO2 Max HIIT Protocol (Norwegian 4×4 method):
4 rounds × 4 minutes at 85–95% maximum heart rate
3 minutes of active recovery (easy walking or jogging) between intervals
Total session: approximately 28–30 minutes including warm-up and cool-down
Frequency: 2× per week is the most researched effective approach
Zone 2 training involves sustained aerobic exercise at a comfortable, conversational pace — typically 60–70% of maximum heart rate, or the intensity at which you can speak in short sentences but not hold a fully comfortable conversation.
Zone 2 training primarily develops the peripheral component of VO2 max — increasing mitochondrial density, capillary density, and fat oxidation capacity. It is less acute as a central cardiac stimulus than HIIT, but its lower intensity allows substantially greater weekly training volume, which produces its own meaningful cardiovascular benefits over the long term.
The practical implication: the best training method for improving VO2 max is the one you can perform consistently at sufficient volume. HIIT may produce faster initial results — but if the intensity creates excessive fatigue, injury risk, or reduces training adherence, Zone 2 training at higher weekly volume will likely produce superior long-term VO2 max development.
Heart Rate Training Zones: A Practical Reference
Maximum Heart Rate Estimate: 208 – (0.7 × age) is more accurate than the commonly cited 220 – age formula
Zone 1 (recovery): <60% MHR | Zone 2 (aerobic base): 60–70% MHR
Zone 3 (tempo): 70–80% MHR | Zone 4 (VO2 max work): 80–90% MHR
Zone 5 (maximal): 90–100% MHR
Interval Training Variations Beyond the 4×4 Protocol
While the Norwegian 4×4 protocol is the most researched format, other interval structures also produce meaningful VO2 max improvements and provide variety within a training program:
Rotating between these formats across a training block prevents accommodation and provides variety that supports long-term training adherence.
Nutrition Timing Around VO2 Max Training Sessions
High-intensity interval training and longer Zone 2 sessions both have meaningful nutritional considerations:
Before HIIT (1–3 hours prior): A mixed meal with carbohydrates supports the glycolytic (carbohydrate-burning) energy demands of near-maximal intervals — going into high-intensity work with low glycogen availability significantly reduces interval quality
Before Zone 2 (1–2 hours prior): A lighter meal is appropriate — Zone 2 training relies more heavily on fat oxidation and tolerates a lower carbohydrate state better than HIIT
After sessions: 20–40 g of protein within 1–3 hours supports muscle repair — aerobic training still stimulates muscle protein synthesis in the trained muscles
These are general guidelines — individual nutritional needs vary based on body size, training history, and any specific dietary requirements. A registered dietitian can provide personalized guidance for optimizing nutrition around VO2 max training.
VO2 Max Training Programs by Fitness Level
For Beginners: The 8-Week Foundation Program
Beginners should not start with HIIT — the cardiovascular and musculoskeletal systems need a base of aerobic fitness before high-intensity interval work can be safely and productively performed.
Weeks 1–2: 20 min Zone 2 walking or easy jog × 3/week Weeks 3–4: 25–30 min Zone 2 × 3/week + 1 light interval session (4–6 × 1 min easy run, 1 min walk) Weeks 5–6: 30 min Zone 2 × 3/week + 1 moderate interval session (5–6 × 2 min moderate effort, 2 min walk) Weeks 7–8: 30 min Zone 2 × 2/week + 2 moderate interval sessions per week
For Intermediate Trainees: Structured Development
Session Type
Protocol
Frequency
Target Intensity
Long Zone 2
40–60 min easy cardio
2× per week
60–70% MHR
VO2 Max Intervals
4–5 × 3–4 min hard, 3 min recovery
1–2× per week
85–95% MHR
Tempo Session
20–30 min comfortably hard
1× per week
75–85% MHR
How Much Can VO2 Max Improve?
Sedentary beginners: 15–30% improvement over 12–16 weeks — the highest gains occur from the lowest baseline
Recreationally active adults: 8–15% improvement with structured training
Already well-trained individuals: 3–8% — improvements become smaller as the trainable ceiling is approached
These ranges represent common outcomes — individual variation based on genetics, training history, age, and program adherence is significant.
Cardiovascular Safety Considerations
⚠️ Before beginning structured HIIT, consult a physician if:
→ You are over 40 and have been sedentary for 6+ months
→ You have known or suspected cardiovascular disease
→ You have risk factors: hypertension, diabetes, high cholesterol, or family history of heart disease
→ You experience chest pain, unusual shortness of breath, or dizziness during exercise
Practical Questions About VO2 Max
Do I need a lab test to know my VO2 max?
Laboratory testing on a treadmill or cycle ergometer with expired gas analysis provides the most accurate measurement. This is available at sports performance centers, university exercise labs, and some sports medicine clinics. Several field estimates are also available — the Cooper 12-minute run test, the Rockport Walk Test, and GPS watch estimates — but these have meaningful error margins compared to laboratory testing. For most recreational exercisers, monitoring training zones using heart rate and perceived effort is sufficient — precise VO2 max values are most valuable for competitive athletes.
Can strength training improve VO2 max?
Traditional resistance training alone produces modest VO2 max improvements in previously sedentary individuals but significantly less than dedicated aerobic training at comparable time investment. Circuit-style resistance training with minimal rest periods may produce moderate VO2 max improvements alongside strength gains. For a primary goal of improving VO2 max, dedicated aerobic training (Zone 2 and HIIT) is considerably more time-efficient than resistance training alone.
✅ Key Takeaways
VO2 max is among the most evidence-supported modifiable predictors of both athletic performance and long-term cardiovascular health
Both HIIT and Zone 2 training improve VO2 max — the best method is whichever you can perform consistently at sufficient volume
Long-interval HIIT (4 min work at 85–95% MHR with 3 min recovery, 2× per week) is the most researched effective protocol
Most sedentary adults can improve VO2 max by 15–30% with 12–16 weeks of structured aerobic training
Consult a sports medicine physician or exercise physiologist for personalized testing if you have cardiovascular health concerns before beginning high-intensity training
Choosing the Right Cardio Mode for VO2 Max Training
VO2 max training principles apply across all aerobic exercise modalities — the specific mode matters less than the intensity and volume principles:
Running: Highest VO2 max stimulus per unit time for most people — more muscle mass engaged than cycling or rowing
Cycling: Lower impact — suitable for those with joint concerns; slightly lower VO2 max stimulus than running at equivalent perceived effort for most individuals
Rowing: High total body engagement — effective VO2 max training with additional upper body and core demand
Swimming: Full body, non-weight-bearing — excellent option for those with lower extremity injuries or joint conditions
Jump rope: Time-efficient, portable — can reach Zone 4 quickly and is particularly effective for HIIT formats
Choose the modality that allows consistent, high-quality training over months — injury avoidance and training adherence are more important for long-term VO2 max development than choosing the theoretically optimal mode.
VO2 Max Development in Masters Athletes (40+)
A question frequently asked by older fitness trainees: is improving VO2 max still worthwhile after 40 or 50?
The answer from the research literature is clearly yes. While absolute VO2 max values are lower in older adults than in their younger counterparts with equivalent training, the relative improvement from aerobic training remains meaningful at any age:
Adults in their 60s and 70s can still achieve 10–20% VO2 max improvements from a structured aerobic training program
The health implications of VO2 max improvements may actually be more significant for older adults than younger ones — given that baseline cardiorespiratory fitness is more often a clinically relevant health concern in this age group
Exercise intensity can typically be safely maintained in healthy older adults — the same Zone 4 training principles apply, with appropriate medical screening and program design
Older adults should seek medical clearance from a physician before beginning a structured high-intensity cardiovascular training program — but the absence of this clearance should be sought, not assumed. Many older adults with no significant cardiovascular pathology can safely perform HIIT with appropriate program progression and monitoring.
Tracking VO2 Max Progress and Long-Term Cardiovascular Development
Field Tests for Progress Monitoring
Without laboratory testing, standardized field tests performed monthly under consistent conditions allow meaningful progress tracking:
Field Test
Protocol
Progress Indicator
Cooper 12-Minute Run
Maximum distance covered in 12 min on flat surface
Increasing distance at same perceived effort
1.5-Mile Time Trial
Fastest possible 1.5-mile run
Decreasing completion time
Resting Heart Rate
Morning pulse before rising (weekly average)
Gradual decline over months of consistent training
GPS Watch Estimate
Wearable VO2 max estimate from run data
Upward trend (absolute values have ~10–15% margin of error)
Perform these tests under consistent conditions — same time of day, similar weather and recovery status, same route or surface — to make month-over-month comparisons meaningful. These tests work best as relative progress indicators rather than absolute VO2 max values.
When VO2 Max Progress Stalls
After 3–6 months of consistent training, VO2 max improvements typically slow. Common causes and management strategies:
Training accommodation: The body adapts to the specific stimulus — vary interval protocols (shorter/harder vs. longer/moderate), or temporarily increase Zone 2 volume to restart progress
Insufficient intensity: Heart rate monitoring may reveal that “hard” intervals are actually Zone 3 efforts — genuine Zone 4 work requires pushing beyond conversational-hard pace
Insufficient volume: Total weekly aerobic volume often needs to increase as fitness improves for continued VO2 max development
Non-training factors: Chronic stress, poor sleep, or inadequate nutrition can limit VO2 max development regardless of training quality
Lifestyle Factors That Support VO2 Max Development
Sleep: 7–9 hours per night supports the cardiovascular recovery and adaptation process — chronic sleep restriction blunts training response across multiple performance measures
Body composition: VO2 max is expressed relative to body weight — reducing excess body fat while maintaining fitness tends to increase relative VO2 max values
Nutrition: Adequate carbohydrate availability supports high-intensity interval training quality; adequate protein supports the muscular adaptations that accompany aerobic training
VO2 Max Across the Lifespan
VO2 max declines with age even in physically fit individuals — approximately 5–10% per decade, with the rate depending heavily on maintained activity level. The key evidence-based finding: while absolute VO2 max decline is inevitable with aging, the rate of decline is significantly slower in individuals who maintain regular aerobic training compared to those who reduce activity.
This means that consistent aerobic training across decades — not achieving a peak VO2 max and then maintaining it — is the most important factor for long-term cardiorespiratory health and functional capacity in older adulthood. Starting an aerobic training program at any age produces measurable improvements — research consistently shows meaningful VO2 max increases from training in adults in their 60s, 70s, and even 80s.
Integrating VO2 Max Training With Strength Work
For trainees who want to develop both strength and cardiovascular fitness simultaneously, a common effective structure:
Example 5-day concurrent training week:
Mon: Strength (lower body) | Tue: Zone 2 cardio (40 min)
Wed: Strength (upper body) | Thu: VO2 max intervals (4×4 HIIT)
Fri: Strength (full body or lower) | Sat/Sun: Rest or easy Zone 1 activity
Placing HIIT sessions on days away from heavy lower body strength work reduces the interference between strength adaptation and aerobic adaptation — the “interference effect” (the documented reduction in strength gains when combined with high volumes of aerobic training) is minimized when adequate recovery separates the two training stimuli.
Monitoring Signs of Overtraining in Cardio Programs
Aggressive VO2 max programs — particularly those combining high HIIT frequency with high Zone 2 volume — carry a risk of overreaching (short-term accumulated fatigue that impairs performance) or overtraining (a prolonged state of maladaptation to training load).
Signs that training volume or intensity may need reduction:
Resting heart rate elevated 5+ beats above normal baseline for multiple consecutive mornings
Performance declining despite consistent training — slower times or higher heart rate at the same pace
Persistent fatigue that does not resolve after a rest day
Mood disturbances, reduced motivation, or increased irritability associated with training
If multiple signs are present, reducing training volume by 40–50% for 1–2 weeks typically allows recovery. Seeking evaluation from a sports medicine physician is recommended if symptoms persist despite rest, as overtraining syndrome requires specific management.
A qualified exercise physiologist or sports performance coach can design a VO2 max development program that accounts for individual fitness level, training history, available time, and any health considerations — producing more consistent improvements than self-directed programming for many intermediate and advanced trainees.
The VO2 Max — Mental Health Connection
An emerging area of research links cardiorespiratory fitness (closely correlated with VO2 max) to cognitive function and mental health outcomes. Aerobic exercise at intensities that challenge VO2 max appears to stimulate BDNF (brain-derived neurotrophic factor — a protein that supports neuron growth and brain plasticity) production, improve neurogenesis (growth of new neurons) in the hippocampus, and produce acute improvements in mood and anxiety.
These cognitive and mental health benefits are a compelling additional rationale for VO2 max training that extends well beyond cardiovascular health and athletic performance — particularly relevant for individuals managing chronic stress, anxiety, or seeking to maintain cognitive function across the lifespan.
While the research on specific dose-response relationships (how much training is needed, at what intensity) for mental health benefits is still developing, the general principle that regular aerobic exercise at meaningful intensities produces both cardiovascular and cognitive benefits is well-supported across multiple independent research lines.
Starting From Zero: The Most Important Step
For completely sedentary individuals beginning aerobic training for the first time (or returning after a long break), the most important principle is starting conservatively and building gradually — not pursuing the most aggressive protocol available.
Beginning with 20–30 minutes of brisk walking three times per week, then progressively increasing duration and eventually intensity over 4–8 weeks, produces consistently better long-term outcomes than immediately attempting HIIT protocols. The initial weeks of aerobic training in a deconditioned individual produce rapid VO2 max improvements even at moderate intensities — aggressive early intensity is not necessary for meaningful progress and significantly increases injury and dropout risk.
The single most evidence-supported strategy for long-term VO2 max development is finding aerobic activities you can sustain consistently over years — not optimizing the training protocol for maximum short-term gain.
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. Why Two Straps Changed What I Thought Training Equipment Needed to…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Exercise carries inherent risks. Always consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program, especially if you have a pre-existing medical condition, injury, or health…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…
⚠️ Health & Fitness Disclaimer This article is for general educational and informational purposes only. It does not replace professional medical or fitness advice. If you have any pre-existing condition, injury, or health concern — please consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program. The cable fly…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Cardiovascular Health Notice: If you have a history of heart disease, high blood pressure, or any cardiovascular condition, obtain…




")







