
Shoulder Mobility: The Research Behind Restricted Range, 6 Key Exercises, and a Progressive 8-Week Plan
Shoulder stiffness rarely announces itself with pain. It shows up as a pressing limitation, an overhead position that feels blocked, or a rack position that never quite works no matter how much you practise.
Most trainees treat shoulder mobility as a warmup afterthought: a few arm circles before training, a brief band stretch after. The shoulder gets progressively stiffer. The limitation compounds into technique problems, then into overuse injuries that take months to resolve.
This guide covers what the research shows about why shoulder mobility becomes restricted, which structures are actually involved, six exercises that address each restriction systematically, and an 8-week progressive plan that produces measurable range of motion improvements.
Why Shoulder Mobility Becomes Restricted: The Structural Causes
The Glenohumeral Joint: Where Most Restriction Originates
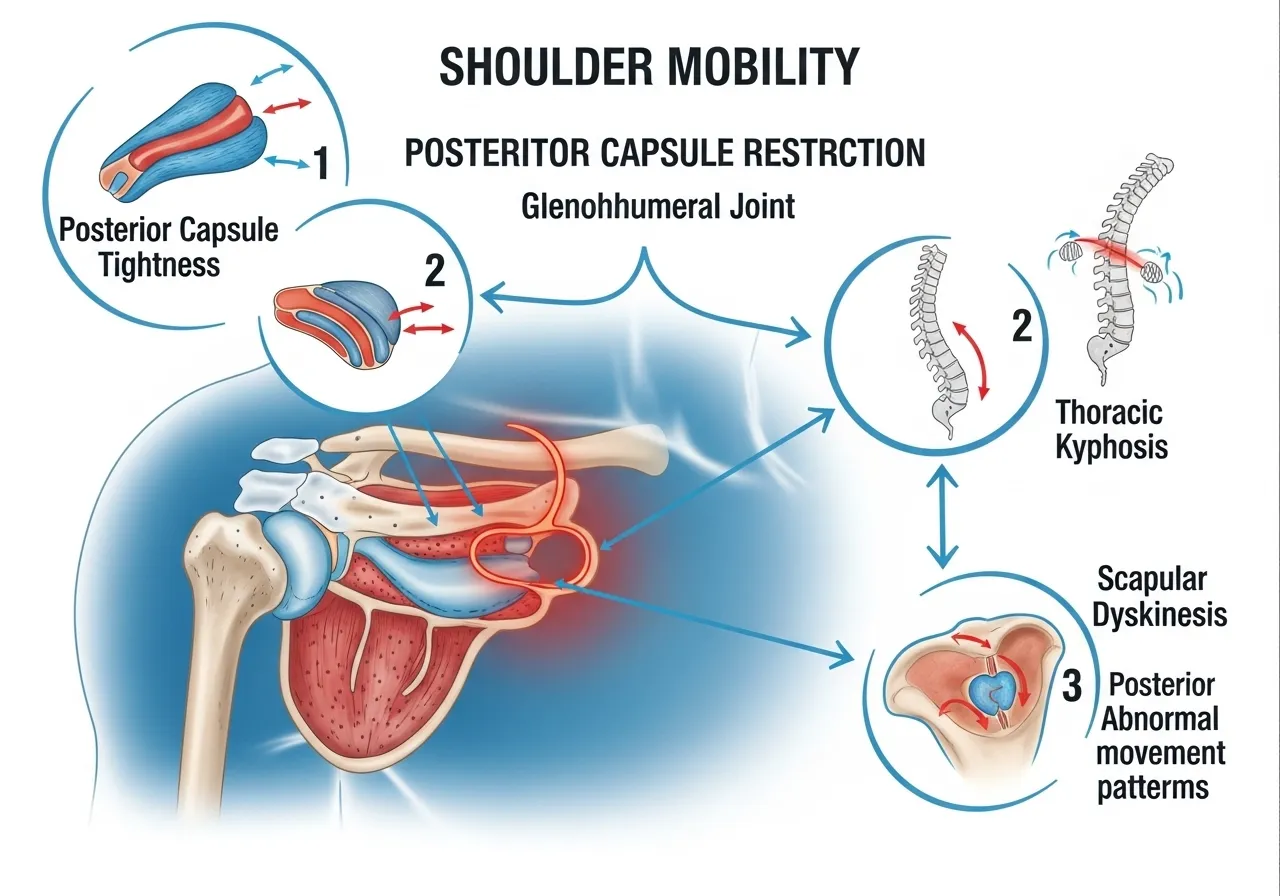
The glenohumeral joint, where the upper arm bone meets the shoulder socket, provides most of the shoulder’s range of motion. It is a ball-and-socket joint with exceptional mobility and correspondingly limited bony stability.
This mobility-stability trade-off means that soft tissue structures, specifically the joint capsule, rotator cuff, and surrounding musculature, provide most of the stability. When these structures become tight, shortened, or scarred from previous injury or disuse, range of motion decreases.
The posterior capsule is the most common site of glenohumeral restriction in strength athletes. Repeated pressing and pulling under load compresses the posterior capsule over time, reducing internal rotation and horizontal adduction. The result: the classic “shoulder impingement” presentation that is often blamed on the rotator cuff when the primary cause is posterior capsule tightness.
The Overhead Range Requirement: What Research Defines
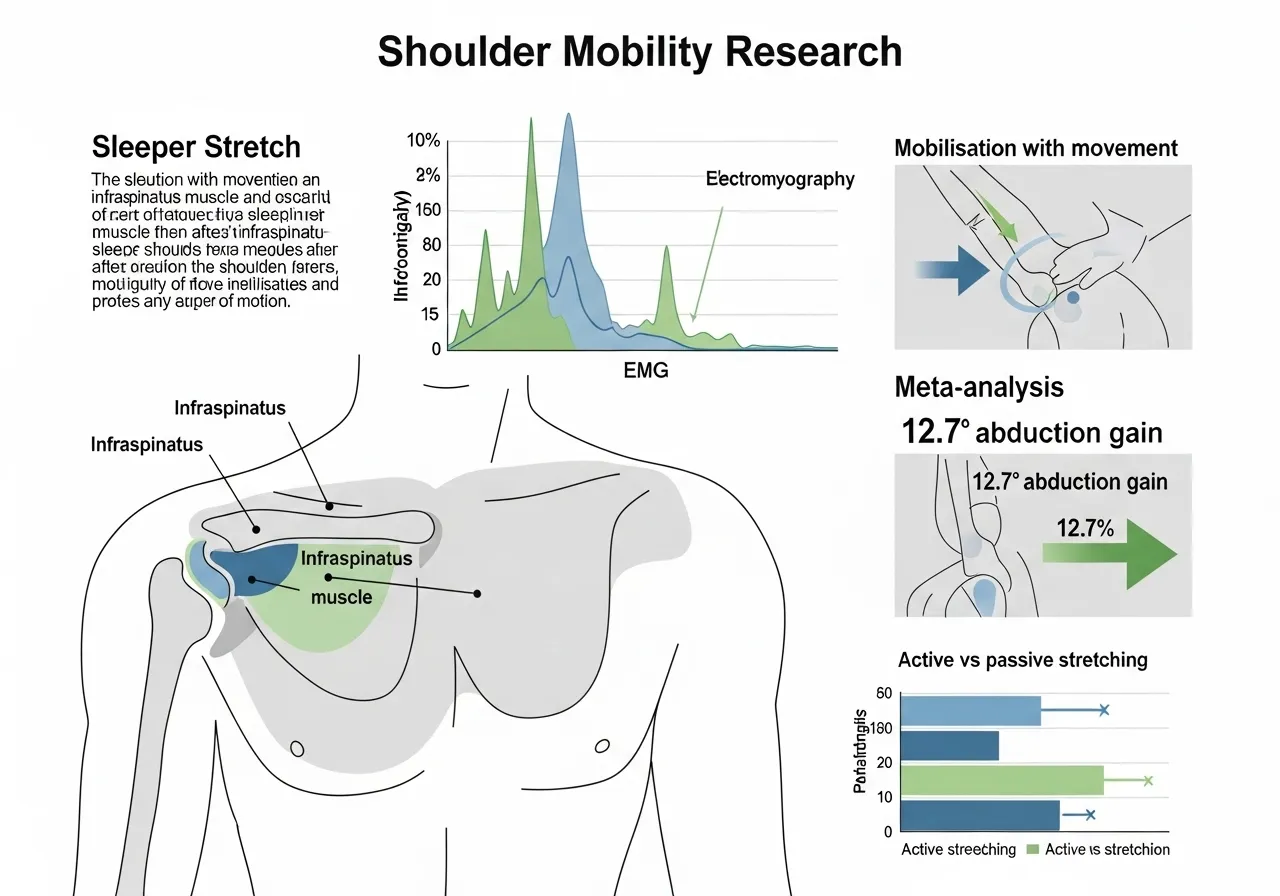
A study clarifying the glenohumeral range of motion required for overhead shoulder mobility found that self-stretching combined with mobilisation could be a useful exercise for shoulder range of motion recovery in individuals with glenohumeral internal rotation deficits, with the intervention producing clinically significant improvements in passive internal rotation compared to control conditions across a randomised controlled trial.
Glenohumeral internal rotation deficit (GIRD) responds to targeted self-stretching combined with mobilisation. Passive stretching alone is frequently insufficient for restoring full glenohumeral range when the posterior capsule is the limiting structure.
The Thoracic Spine Connection
The shoulder does not move in isolation. Every overhead and pressing movement involves a coordinated sequence across the glenohumeral joint, scapulothoracic joint, sternoclavicular joint, and acromioclavicular joint.
Thoracic kyphosis, the rounding of the upper back that accumulates from desk-based work, directly limits this coordinated sequence. A rounded upper back repositions the scapula into a downwardly rotated and protracted position. This reduces the subacromial space and limits glenohumeral elevation before the joint even begins its range. Addressing thoracic extension is therefore not optional in shoulder mobility work. It is foundational. For a complete programme targeting thoracic restriction, the thoracic mobility guide covers the upstream causes that compound glenohumeral restriction.
The Scapular Component
The scapula must upwardly rotate as the arm elevates overhead. If the serratus anterior and lower trapezius are weak or inhibited, the scapula does not rotate adequately. The arm elevation is then achieved by the glenohumeral joint compensating beyond its intended range, creating impingement rather than clean overhead movement.
This is why isolated glenohumeral stretching often fails to resolve overhead shoulder restrictions. The scapular stabilisers must be addressed simultaneously. The scapular stability guide covers the serratus anterior and lower trapezius exercises that restore scapular upward rotation and directly improve overhead shoulder range.
What the Research Shows About Shoulder Mobility Interventions
Sleeper Stretch and Thoracic Manipulation: Combined EMG Evidence
A randomised study assessing the effects of adding thoracic manipulation to posterior glenohumeral mobilisations and sleeper stretches in shoulders with decreased internal rotation found that adding thoracic manipulation to posterior glenohumeral mobilisation and sleeper stretches produced greater improvements in passive range of motion and infraspinatus electromyographic activity compared to mobilisation and stretching alone, suggesting that addressing the thoracic spine as part of shoulder mobility interventions produces superior outcomes to treating the glenohumeral joint in isolation.
Adding thoracic manipulation to glenohumeral stretching produces greater range of motion gains and better infraspinatus activation than glenohumeral stretching alone. Shoulder mobility is a regional, not a local, problem.
Mobilisation With Movement: Meta-Analysis Evidence
A systematic review and meta-analysis of 26 studies investigating mobilisation with movement on shoulder pain and range of motion found that mobilisation with movement improved pain during movement with a moderate effect size and shoulder abduction range of motion by 12.7 degrees compared to sham conditions in the short term, with combined mobilisation with movement and conventional rehabilitation improving pain at rest, disability, and both shoulder abduction and external rotation compared to conventional rehabilitation alone.
Active mobilisation combined with movement outperforms passive stretching alone for restoring shoulder abduction and external rotation range. Loading the tissue while moving through range produces superior adaptations to stretching at rest.
Why Static Stretching Alone Is Often Insufficient
Static stretching improves flexibility by reducing the stretch reflex threshold and increasing stretch tolerance. For general muscle tightness, it works. For joint capsule restriction, it is less effective because the joint capsule is not a muscle. It does not respond to the stretch reflex mechanism.
Posterior capsule tightness requires a different input: low-load, sustained positional stretching that creates a creep deformation in the capsular tissue over time. The sleeper stretch and cross-body stretch work on this principle. They create sustained compression of the posterior capsule in a position that gradually lengthens it over weeks of consistent practice, not sessions of intense stretching.
The evidence consistently shows that frequency and consistency of application matter more than intensity of stretch. Three minutes of posterior capsule stretching daily produces greater improvements than ten minutes twice per week at the same total weekly volume.
Diagnosing Your Specific Shoulder Mobility Restriction
The 3 Primary Restriction Patterns
Shoulder mobility restrictions fall into three primary patterns with distinct causes and distinct corrective approaches. Identifying which pattern applies before beginning any exercise programme prevents months of incorrect work:
| Restriction Pattern | Primary Symptom | Likely Cause | Primary Fix |
|---|---|---|---|
| Internal rotation deficit | Cannot reach up the back, front rack collapses | Posterior capsule tightness | Sleeper stretch, cross-body stretch |
| External rotation deficit | Overhead press flares, elbows flare wide | Subscapularis and anterior capsule tightness | Doorframe stretch, banded external rotation |
| Elevation deficit | Arms cannot reach overhead cleanly, impingement pain at top | Scapular dyskinesis and thoracic kyphosis | Thoracic extension, serratus activation |
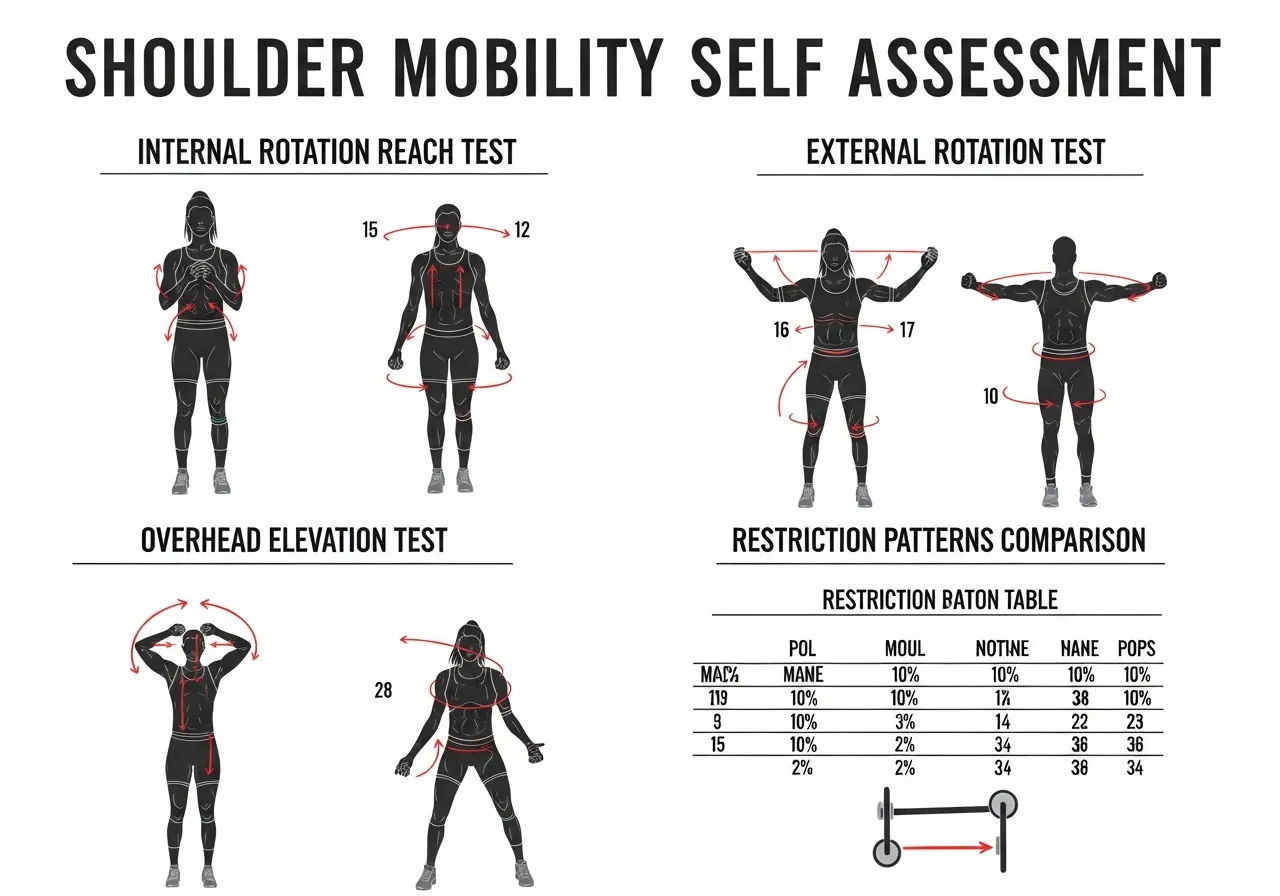
Self-Assessment: The 3 Tests
Test 1 (Internal rotation): Reach your hand up your back toward the opposite shoulder blade. A normal internal rotation range allows the thumb to reach at least the level of T7, the mid-thoracic spine. If you cannot reach the low back, glenohumeral internal rotation is significantly restricted.
Test 2 (External rotation): Stand with your upper arm at your side, elbow at 90 degrees, and rotate your forearm outward. Normal external rotation at the side is 60 to 90 degrees. If your forearm cannot reach 60 degrees from neutral without the elbow drifting away from the body, anterior capsule or subscapularis tightness is the limiting factor.
Test 3 (Overhead elevation): Lie flat on your back with arms at your sides. Keeping the lower back in contact with the floor, raise both arms overhead and attempt to touch the floor behind your head. If you cannot reach the floor or the lower back arches significantly during the attempt, thoracic kyphosis or shoulder capsule restriction is limiting overhead elevation.
Why Most Trainees Have Multiple Patterns Simultaneously
The internal rotation deficit, external rotation deficit, and elevation deficit are not mutually exclusive. Strength athletes who press and pull frequently typically develop posterior capsule tightness from loading and anterior capsule tightness from the protracted shoulder position that accumulates during desk work.
The result: both internal and external rotation are restricted, with elevation limited by scapular positioning on top. The correction requires addressing all three patterns simultaneously rather than treating one and waiting for results before addressing the next.
6 Key Shoulder Mobility Exercises: Targets, Technique, and Progressions
These exercises address mobility restriction in healthy shoulders. Individuals with diagnosed rotator cuff tears, labral tears, shoulder instability, or recent shoulder surgery should obtain physiotherapy assessment and clearance before performing any of the mobility exercises below. Sharp pain rather than stretch sensation during any exercise is a signal to stop immediately.
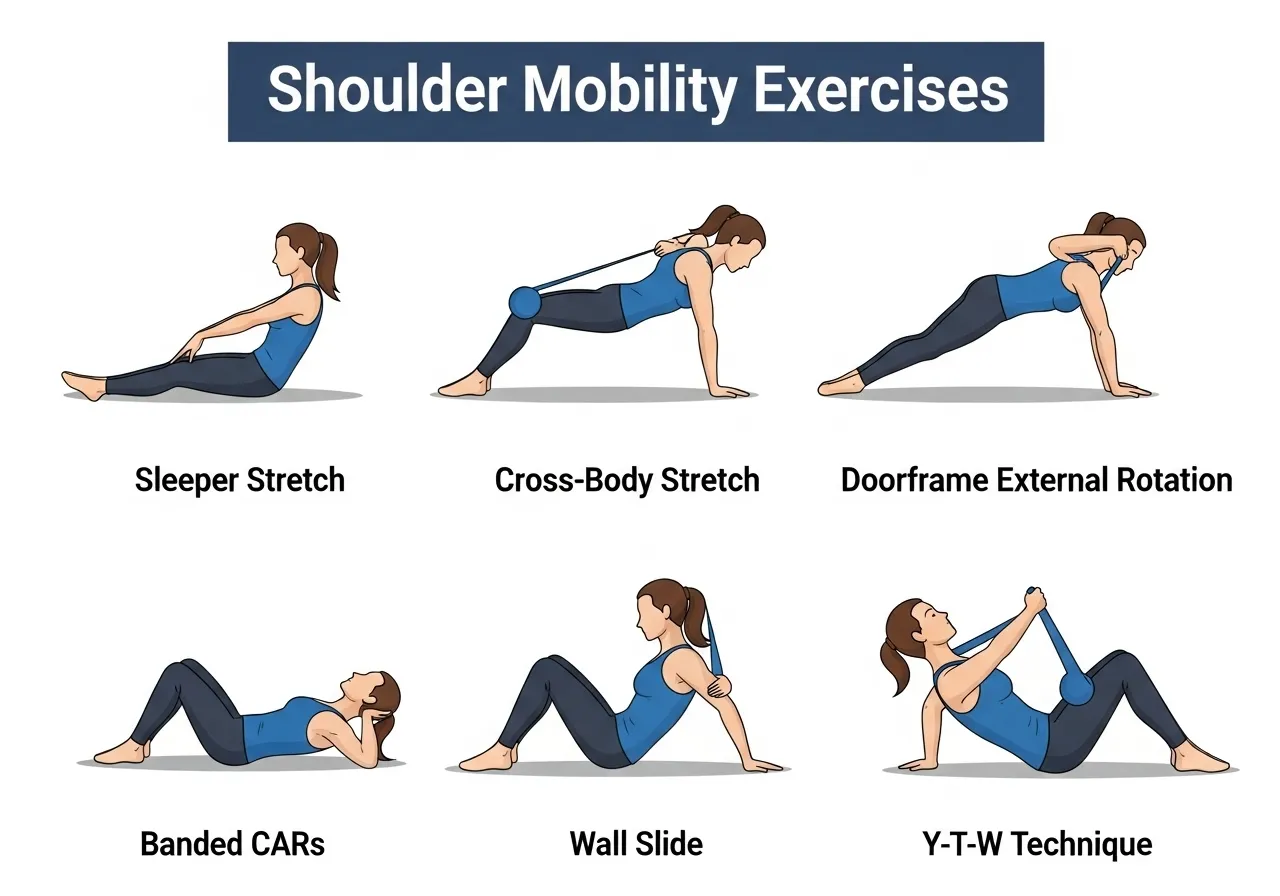
🔵 1. Sleeper Stretch
Target: Posterior glenohumeral capsule, internal rotation range
How: Lie on your side with the target shoulder on the floor, upper arm parallel to the floor and elbow at 90 degrees. Use the opposite hand to gently press the forearm toward the floor, rotating the shoulder internally. Hold for 30 to 60 seconds. Do not allow the shoulder blade to lift off the floor during the stretch.
Key point: The stretch should be felt in the back of the shoulder, not the front. If you feel anterior shoulder pinching, reduce the range until the sensation moves posterior. Frequency matters more than intensity: perform daily rather than intensely twice per week.
🔵 2. Cross-Body Stretch
Target: Posterior glenohumeral capsule, horizontal adduction range
How: Bring the target arm across the body at shoulder height. Use the opposite hand to apply gentle pressure above the elbow (not at the wrist) and draw the arm further across the chest. Hold 30 seconds. Keep the shoulder blade down and back throughout.
Key point: This stretch targets the same posterior capsule as the sleeper stretch but from a standing position. Use both exercises in combination. The cross-body stretch is more accessible during training warmups; the sleeper stretch allows better scapular stabilisation during the stretch.
🔵 3. Doorframe External Rotation Stretch
Target: Anterior capsule, subscapularis, external rotation range
How: Stand in a doorframe with the upper arm at shoulder height and elbow at 90 degrees. Place the forearm against the doorframe. Rotate the body away from the arm until a stretch is felt in the front of the shoulder. Hold 30 seconds. Perform at two to three heights (low, middle, high) to address different portions of the anterior capsule.
Key point: Keep the shoulder blade retracted throughout. If the shoulder blade protracts as you rotate away, you are stretching the pectoralis minor rather than the anterior capsule. Pull the shoulder back before applying rotation.
🔵 4. Banded Shoulder CARs (Controlled Articular Rotations)
Target: Full glenohumeral range, articular cartilage health, neuromuscular awareness
How: With a light band attached at elbow height, hold the band and perform slow, deliberate circles with the shoulder through its full available range. Move as far as control allows in each direction. The band provides proprioceptive feedback and mild traction that helps the joint move through restricted ranges more comfortably.
Key point: Speed is the enemy of CARs. A single full rotation should take 8 to 10 seconds. Moving slowly keeps the movement under active neuromuscular control rather than momentum. This is the single most important exercise for maintaining shoulder joint health over time.
🔵 5. Wall Slide with Overhead Reach
Target: Serratus anterior, lower trapezius, scapular upward rotation, overhead elevation
How: Stand facing a wall with forearms flat against it at shoulder height. Keeping the forearms in contact with the wall, slide both arms overhead as far as range allows. At the top, push the forearms gently into the wall to activate the serratus anterior. Slowly return to the start position.
Key point: The wall slide is not a passive stretch. It is an active mobility exercise that trains the scapular upward rotation needed for clean overhead elevation. If the lower back arches significantly during the slide, thoracic mobility is the limiting factor rather than glenohumeral restriction.
🔵 6. Prone Y-T-W Raises
Target: Lower trapezius, middle trapezius, posterior deltoid, scapular retraction and depression
How: Lie face down on a bench or floor. Raise both arms into the Y position (overhead at 30 degrees from the midline), then T position (directly to the sides at 90 degrees), then W position (elbows at 90 degrees, hands forward). Hold each position for 2 seconds at the top. Use bodyweight only or very light load initially.
Key point: The Y-T-W sequence addresses the lower and middle trapezius that almost every strength athlete underloads. Weakness in these muscles is the structural cause of the rounded shoulder posture that limits overhead range. Strengthening them alongside stretching the anterior structures produces lasting positional change.
The 4 Shoulder Mobility Mistakes That Keep Trainees Stuck
Mistake 1: Only Stretching, Never Strengthening
The most common shoulder mobility error is treating the problem as purely a flexibility deficit. Trainees stretch the posterior capsule, do doorframe stretches, and foam roll the thoracic spine. The range of motion improves temporarily and returns to its restricted baseline within 24 to 48 hours.
The reason: a restricted shoulder is almost always accompanied by weakness in the muscles that should stabilise the new range of motion. The nervous system returns to the restricted position because it does not trust the musculature to control the expanded range.
The fix is to pair every stretching exercise with a strengthening exercise for the muscles that should own that range. Sleeper stretch for internal rotation is paired with external rotation strengthening. Wall slides for overhead elevation are paired with Y-T-W raises for lower trapezius strength. Mobility without stability does not persist.
Mistake 2: Aggressive Intensity Over Consistent Frequency
The shoulder capsule is dense connective tissue. It responds to low-load, sustained pressure over time, not to intense, infrequent stretching bouts.
Trainees who perform aggressive shoulder stretching once or twice per week and feel sore afterward are creating micro-inflammation in the capsular tissue. This inflammation temporarily reduces range of motion before it resolves, and the capsule may remodel to a thicker, stiffer state over months of this pattern.
The correct approach: three to five minutes of posterior capsule stretching daily at a comfortable tension, not an aggressive one. The cumulative effect of daily low-load application exceeds the effect of intense, infrequent bouts for capsular tissue remodelling.
Mistake 3: Ignoring the Thoracic Spine
Trainees who address the glenohumeral joint in isolation while ignoring the thoracic spine consistently plateau at partial improvements. The scapula cannot upwardly rotate properly on a kyphotic thoracic spine. The glenohumeral joint cannot achieve full elevation if the scapular platform is positioned incorrectly.
Five minutes of thoracic extension work before shoulder mobility exercises changes the outcome for most trainees. The scapula repositions, the subacromial space opens, and the glenohumeral exercises produce their full effect instead of a fraction of it.
Mistake 4: Stopping When Symptoms Resolve
Most trainees stop shoulder mobility work when the pressing pain or overhead restriction improves. This is the point where the work actually begins producing structural change rather than symptomatic relief.
Capsular tissue remodelling takes six to twelve weeks of consistent intervention to produce lasting change. Symptom resolution occurs at two to four weeks. Stopping at symptom resolution means stopping before the structural change is complete, which is why the restriction returns within months of discontinuing the programme.
Maintaining two to three minutes of posterior capsule work and wall slides daily as permanent training practice. This prevents restriction from re-accumulating. For a broader framework covering all four major mobility areas, the mobility training guide covers the complete protocol.

8-Week Shoulder Mobility Programme: Progressive Structure
📅 Phase 1: Weeks 1 to 2: Assessment and Foundation
- Complete the 3 self-assessment tests to identify primary restriction patterns
- Sleeper stretch: 2 sets of 45 seconds daily
- Cross-body stretch: 2 sets of 30 seconds daily
- Doorframe stretch at 3 heights: 30 seconds each daily
- Wall slide: 3 sets of 8 reps, 2 seconds hold at top, daily
Focus: Establish baseline, begin daily capsule stretching habit. Do not skip days. Frequency is the active ingredient in Phase 1.
📅 Phase 2: Weeks 3 to 4: Adding Active Mobility
- Continue all Phase 1 exercises
- Add banded shoulder CARs: 5 slow circles each direction, twice daily
- Add Y-T-W raises: 3 sets of 10 reps each position, 3 times per week
- Thoracic extension over foam roller: 2 minutes pre-session
Focus: Begin training neuromuscular control of the new range. The CARs convert passive range gained in Phase 1 into active, usable range.
📅 Phase 3: Weeks 5 to 6: Load the Range
- Maintain all stretching at Phase 1 and 2 volumes
- Y-T-W raises: progress to light plate or band resistance
- Add band pull-apart: 3 sets of 15 reps, focus on full external rotation at end range
- Add overhead reach holds: standing, reaching both arms to full overhead range and holding 5 seconds, 5 reps
Focus: Begin loading the expanded range to signal to the nervous system that the new position is safe and stable.
📅 Phase 4: Weeks 7 to 8: Integration and Maintenance Standard
- Reduce stretching to maintenance volume: sleeper stretch and cross-body stretch once daily
- Maintain Y-T-W and band pull-apart as permanent training accessories
- Re-test the 3 self-assessment tests: measurable improvements in all 3 patterns expected
- Integrate overhead reach holds as warmup before all pressing sessions
Focus: Establish the maintenance standard that prevents restriction from re-accumulating. The goal of Phase 4 is not to keep improving but to make Phase 3 results permanent.
Frequently Asked Questions About Shoulder Mobility
How long does it take to improve shoulder mobility?
Noticeable symptomatic improvement, reduced pressing discomfort and slightly better overhead range, typically occurs within two to four weeks of consistent daily work.
Measurable range of motion change on standardised testing typically requires six to eight weeks. Structural capsular remodelling that produces lasting, permanent change without maintenance intervention takes twelve or more weeks of consistent application.
Should I work on shoulder mobility before or after training?
Active mobility work, wall slides, banded CARs, and overhead reach holds, belongs before training. These exercises prepare the shoulder for its working range and improve neuromuscular activation patterns that enhance pressing and pulling performance.
Passive capsule stretching, sleeper stretch and cross-body stretch, is most effective after training when the tissues are warm, or as a standalone session before sleep. Performing passive stretching immediately before heavy loading may transiently reduce force output.
Is shoulder clicking or popping a sign of mobility restriction?
Painless clicking or popping during shoulder movement is typically cavitation, the release of gas from the joint space, or tendon snapping over a bony prominence. It is not inherently pathological and does not require treatment.
Painful clicking, especially clicking accompanied by a catching sensation, apprehension, or weakness, indicates a structural issue including a labral tear or rotator cuff pathology that requires professional assessment before mobility work continues.
Can shoulder mobility work help with bench press shoulder pain?
In many cases yes, but the response depends on the cause of the pain. Anterior shoulder pain during bench pressing commonly originates from posterior capsule tightness causing the humeral head to migrate anteriorly under load. Consistent posterior capsule work with the sleeper stretch and cross-body stretch often resolves this pattern within four to six weeks.
If bench press shoulder pain persists after six weeks of systematic posterior capsule and scapular work, professional assessment is warranted to rule out acromioclavicular joint pathology, rotator cuff involvement, or labral irritation that stretching alone cannot address.
How is shoulder mobility different from shoulder stability?
Shoulder mobility refers to the range of motion available at the glenohumeral and scapulothoracic joints, specifically how far the arm can move in each direction. Shoulder stability refers to the neuromuscular control that maintains the humeral head in the correct position within the socket throughout that range of motion.
Both are required for healthy shoulder function. Mobility without stability produces a hypermobile shoulder that is injury-prone. Stability without mobility produces a stiff shoulder that cannot access the range needed for overhead and pressing work. The 8-week programme above addresses both simultaneously by pairing each stretching intervention with a corresponding strengthening exercise.
- The posterior capsule is the most common site of glenohumeral restriction in strength athletes. Daily low-load stretching outperforms intense infrequent stretching for capsular tissue remodelling.
- Adding thoracic manipulation to glenohumeral stretching produces greater range of motion gains and better infraspinatus activation than stretching the shoulder in isolation
- Mobilisation with movement improves shoulder abduction by a mean of 12.7 degrees compared to sham conditions. Active movement through range outperforms passive stretching at rest.
- Every stretching exercise should be paired with a strengthening exercise for the muscles that stabilise the new range. Mobility without stability does not persist.
- Symptom resolution at 2 to 4 weeks is not structural change. Continue the programme for 8 to 12 weeks to produce lasting capsular remodelling.











