⚠️ Shoulder and Rotator Cuff Safety Note The lateral raise elevates the arm through shoulder abduction — a movement that narrows the subacromial space and can provoke impingement in individuals with existing rotator cuff pathology or AC joint irritation. Those with diagnosed supraspinatus tears, active shoulder impingement syndrome, or a history of shoulder surgery should obtain medical clearance before lateral raise training. Pain specifically at the top of the shoulder during abduction is a stop signal. The technique detail of thumb-up versus pinky-up rotation (explained in this guide) significantly affects impingement risk and should be understood before loading the exercise.
The lateral raise is one of the most argued-about exercises in gym culture.
Light weight versus heavy weight. Full range versus partial range. Dumbbell versus cable. Thumb up versus pinky up. Every detail attracts passionate opinions — most of which have not been tested in research.
The EMG and hypertrophy literature on lateral raises is now substantial enough to answer the most important questions with data. This guide covers what the research actually shows about medial deltoid activation, how dumbbell and cable raises compare for muscle growth, what rotation technique does to activation patterns, and how to build a complete shoulder programme around the exercise.
The Lateral Raise Is the Most Important Shoulder Exercise Nobody Programmes Correctly
Why the Lateral Head Makes the Shoulder
The deltoid has three heads: anterior (front), medial (middle), and posterior (rear). Most pressing programmes develop the anterior deltoid heavily — bench press, overhead press, and dips all activate the anterior head significantly. The posterior deltoid gets some work from rows and face pulls.
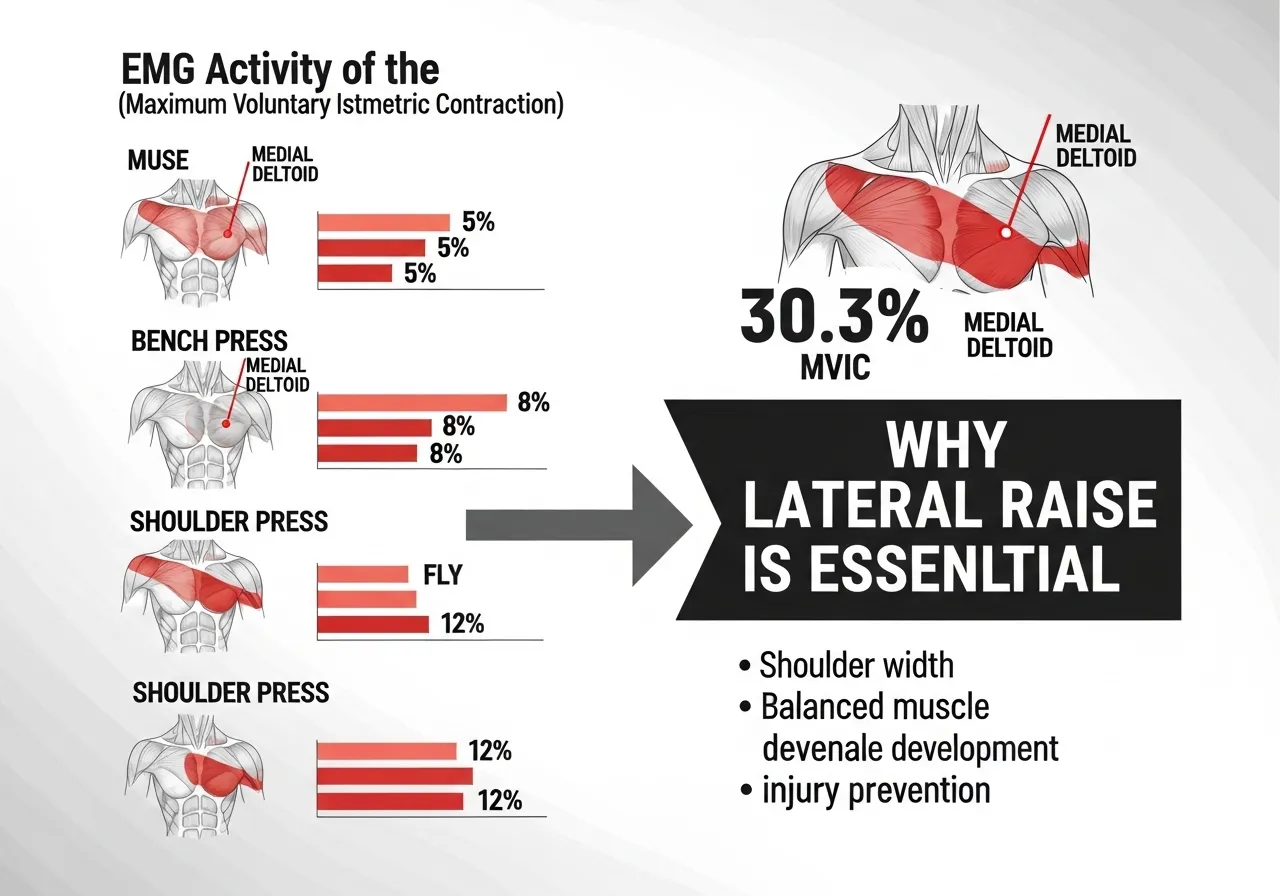
The medial (lateral) deltoid is the head that creates shoulder width — the capped, rounded appearance visible from the front and the side. It receives minimal direct stimulus from pressing or pulling movements. The shoulder press activates the medial deltoid at 27.9% MVIC; the lateral raise activates it at 30.3% MVIC — nearly identical. But the shoulder press also heavily loads the anterior deltoid and triceps, while the lateral raise concentrates the stimulus almost entirely on the medial head.
For trainees who want three-dimensional shoulder development, the lateral raise is not an accessory exercise. It is the primary medial deltoid stimulus — and for that head specifically, no compound exercise replaces it.
The EMG Evidence: Lateral Raise Outperforms Everything for the Medial Deltoid
📌 Key Finding
The lateral raise produces 6× more medial deltoid activation than the bench press and nearly 9× more than the dumbbell fly. No pressing movement substitutes for it — the medial deltoid simply does not receive direct training from compound exercises.
How Much Lateral Raise Volume Do You Actually Need?
The medial deltoid is a relatively small muscle with good recovery capacity. Research on volume-response relationships for isolation exercises suggests 12–20 direct working sets per week produce optimal hypertrophy for most trainees — split across 2–3 sessions.
Many trainees under-programme lateral raises — treating them as an afterthought after pressing work — and wonder why their shoulders lack width. The medial deltoid only grows when it receives sufficient direct volume. Three sets of lateral raises once a week is insufficient for meaningful development in most trained individuals.
Dumbbell or Cable Lateral Raise — Does It Actually Matter for Muscle Growth?
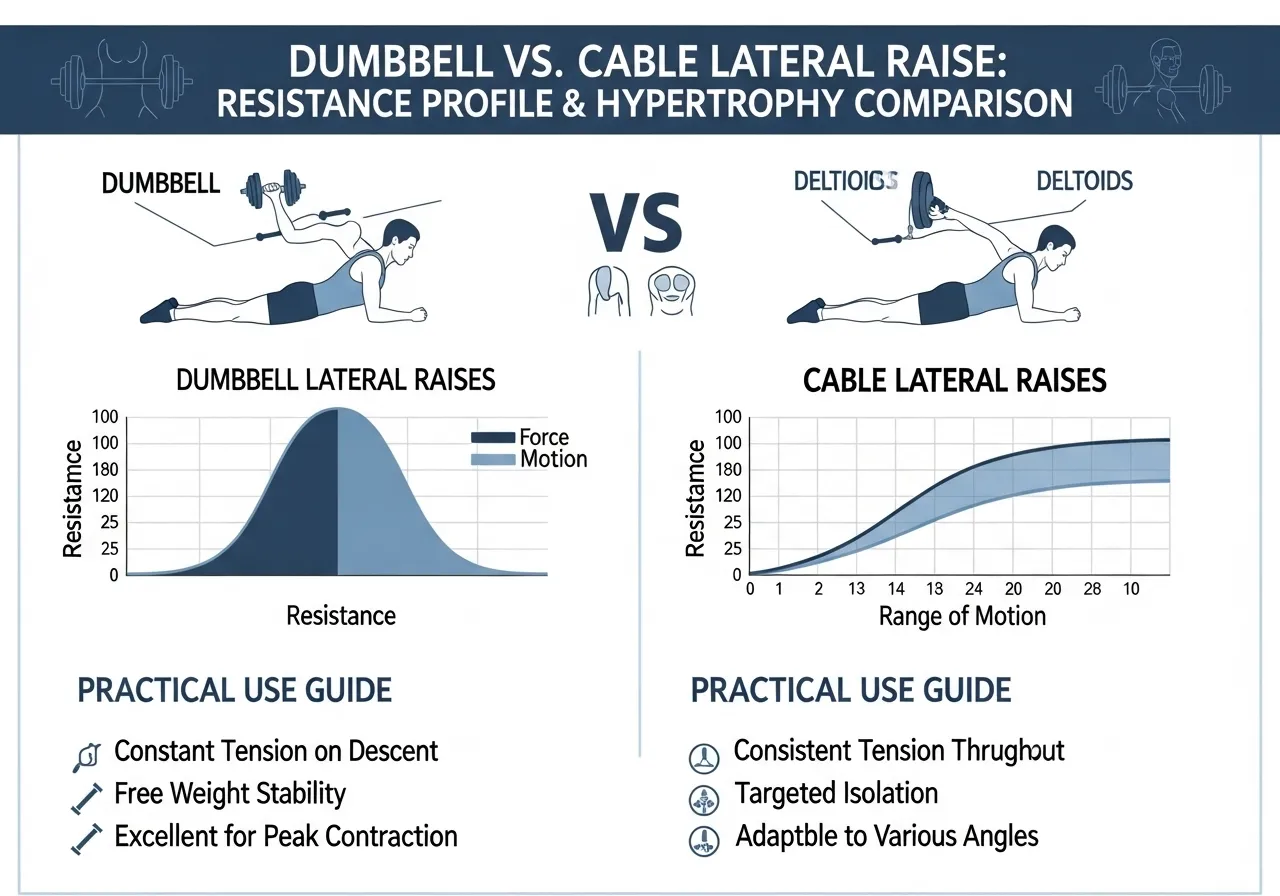
📌 Key Finding Dumbbell = Cable for lateral deltoid hypertrophy. The resistance profile difference (dumbbell peak at 90° vs cable constant tension) does not translate to a measurable difference in muscle growth when volume and proximity to failure are matched.
The Resistance Profile Difference: Why Theory Predicted Cable Would Win
The cable lateral raise was predicted to produce superior hypertrophy based on the lengthened-position loading hypothesis — the idea that muscles grow more when trained at their longest position under the greatest load.
For the lateral deltoid, the lengthened position is at the side of the body (arm adducted). A cable pulled from a low pulley provides resistance throughout this lengthened range. A dumbbell provides near-zero resistance at the side of the body (when the arm is down, gravity acts perpendicular to the lift) — the resistance peaks at 90° where the deltoid is shortened.
Despite this theoretical advantage, the research found no difference. Two explanations are plausible: the lateral deltoid may not respond to lengthened-position loading the way the quads and hamstrings do, or the difference in total mechanical tension across the full range may not be sufficient to create a detectable hypertrophy difference over the intervention period.
Practical Implications: Use Both for Variety
Since neither produces superior hypertrophy, the selection criteria become practical rather than physiological:
Dumbbell: More accessible, allows bilateral training, easier load progression, greater freedom of movement path
Cable (low pulley): Constant tension throughout the range, better feel at the lengthened position, easier to control eccentric phase at low loads, suited for high-rep sets
Rotation principle: Rotating between both across training blocks prevents adaptation to a single resistance profile — providing sensory and mechanical variety without compromising hypertrophy outcomes
Thumb Up vs Pinky Up: How Rotation Angle Changes Everything
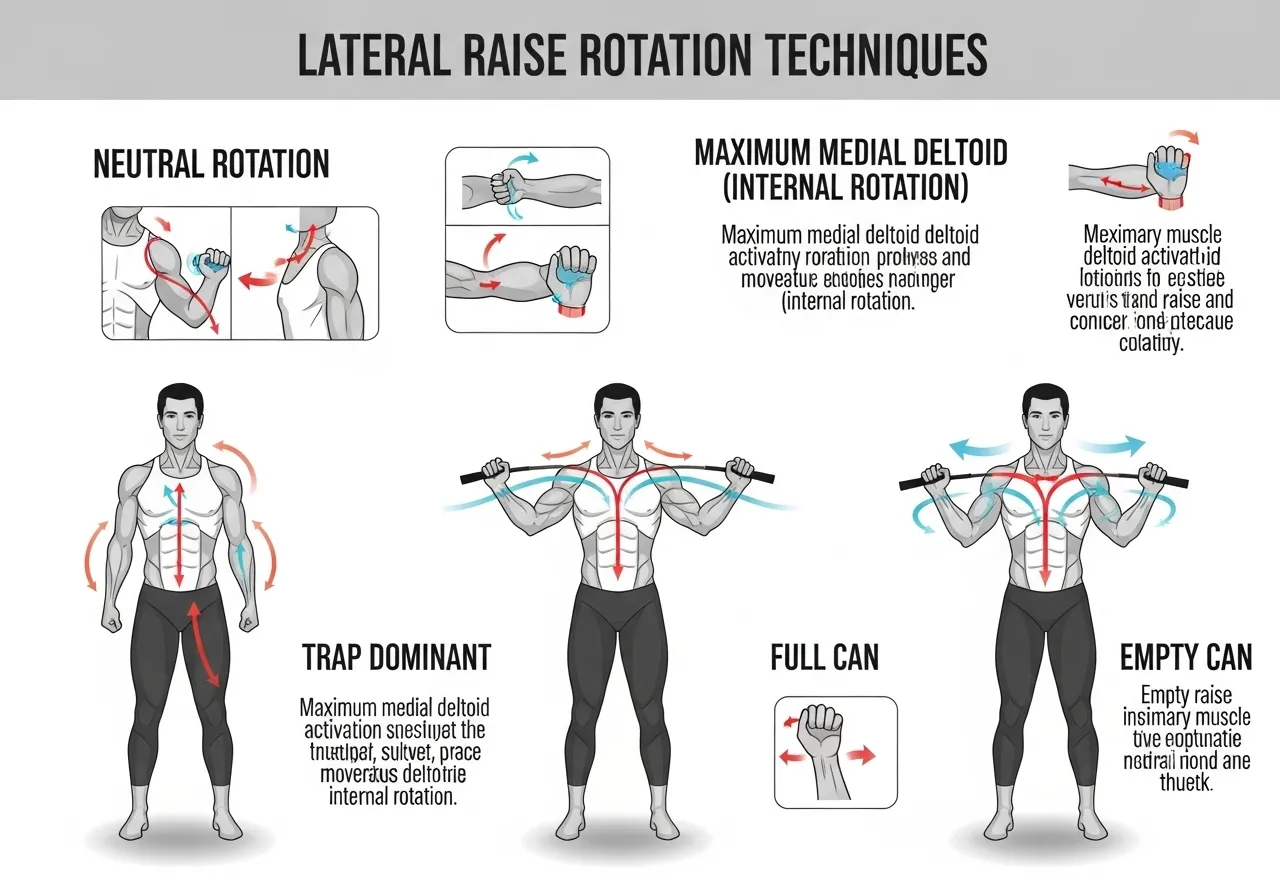
📌 Key Finding Neutral rotation (thumb facing forward) = maximum medial deltoid. Internal rotation (pinky up) = posterior deltoid and upper trap dominant. The common “pinky up” cue shifts activation AWAY from the medial deltoid — the opposite of what most trainees want.
The “Empty Can” Position: What the Research Shows
The “empty can” cue — internally rotating the shoulder during lateral raises (as if pouring a can of liquid) — is one of the most widely taught lateral raise technique cues in gym settings.
The EMG data shows it is the worst cue for medial deltoid development. Internal rotation during abduction shifts the activation profile toward the posterior deltoid and upper trapezius — and more critically, it places the supraspinatus (a rotator cuff tendon) in a position of maximum impingement risk under the acromion.
The research-supported position for maximising medial deltoid activation with minimal impingement risk is neutral or slight external rotation — thumb facing forward or slightly upward throughout the lift. This is sometimes called the “full can” position. It reduces upper trapezius compensation, maximises medial deltoid activation, and keeps the supraspinatus in a less compressed position throughout the abduction range.
The Elbow Angle Consideration
Most lateral raise instruction specifies a slight bend in the elbow — approximately 10–15°. The EMG study found that the flexed-elbow variation (significantly bent arm) reduces medial deltoid activation compared to the near-straight-arm neutral variation.
A slight natural elbow bend during the lift is appropriate to reduce elbow joint stress. Dramatically bending the elbow (45°+) reduces the effective moment arm and shifts the exercise mechanically — not enough to meaningfully change target muscle activation according to current evidence, but also providing no benefit that justifies the reduced ROM. See also: overhead press guide for how lateral raise programming integrates within a complete shoulder session structure.
Lateral Raise Technique: The Details That Determine Whether You Train the Deltoid or the Trap
Setup: Before the First Rep
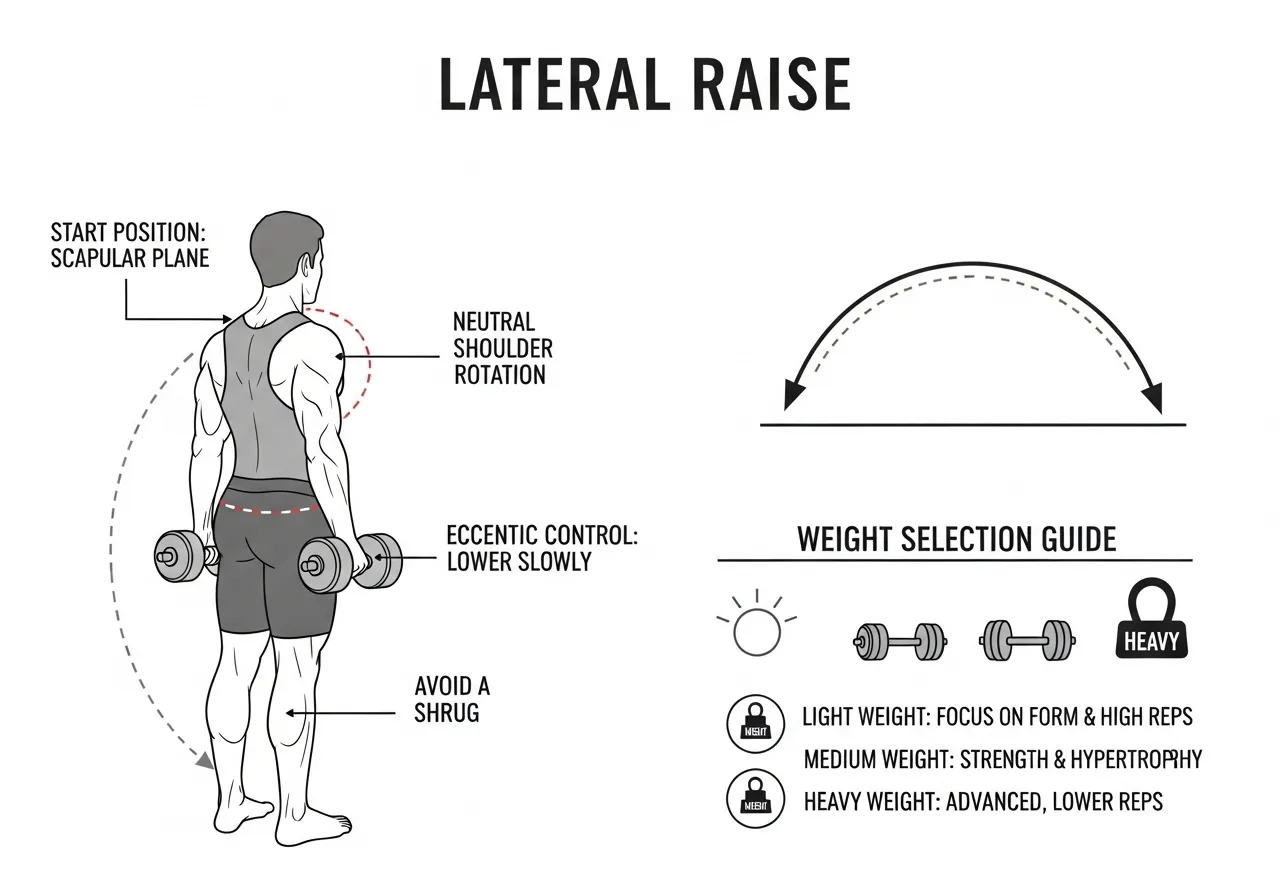
Starting position: Stand or sit upright. Dumbbells at the sides, thumbs facing forward (neutral rotation). A very slight forward torso lean (5–10°) shifts the resistance more directly onto the medial deltoid by aligning the lift direction with the deltoid’s fibre orientation.
Elbow position: Slight natural bend — not locked straight, not aggressively bent. Think of the arm as a lever from shoulder to dumbbell, with just enough elbow bend to reduce joint discomfort.
Shoulder starting point: Begin with arms at the sides, not crossed in front of the body. Some lifters allow the dumbbells to drift forward at the start — this converts the movement toward a front raise and reduces medial deltoid involvement.
Execution: The Lift
Raise the dumbbells outward and slightly forward in the scapular plane — approximately 30° in front of true lateral. The scapular plane (the natural plane of shoulder elevation) produces less impingement than pure frontal plane abduction and feels more natural for most shoulder anatomies.
Raise to approximately ear level — 90° of shoulder abduction, or slightly above. Going significantly above 90° increases upper trapezius involvement without proportionally increasing medial deltoid activation. The medial deltoid reaches its peak activation between 60–90° of abduction.
Resist the temptation to shrug at the top. The shrug — upper trapezius elevation at the end of the raise — is one of the primary compensation patterns that develops when the weight is too heavy or when the shoulder lacks the stability to maintain position at end range.
Eccentric Control: The Most Neglected Component
Most lateral raise reps involve a slow, controlled lift and a fast, uncontrolled lowering. This wastes 50% of the potential hypertrophic stimulus per rep. A deliberate 3-second eccentric (lowering) phase produces significantly greater time under tension for the medial deltoid without changing the load or the number of sets.
The Weight Selection Problem
Lateral raises are systematically overloaded by most trainees. The medial deltoid is a relatively small muscle generating force through a short moment arm. Most trained individuals can genuinely challenge the medial deltoid with 5–12 kg dumbbells in the 12–20 rep range when technique is strict and the eccentric is controlled.
Trainees who use 20–30 kg for lateral raises are typically training their upper trapezius, momentum, and lower back — not their medial deltoid. If you cannot complete the full range without shrugging, the weight is too heavy for the target muscle to control.
Partial Reps at the Lengthened Position: An Evidence-Based Technique
Recent research on lengthened-position training has renewed interest in bottom-range partial reps for lateral raises — performing reps only in the lower half of the range (0–45°), where the deltoid is most lengthened and the cable or dumbbell provides the greatest relative challenge to that range.
While the dumbbell vs cable study found no hypertrophy difference between full-range conditions, both conditions used standardised full ROM. Current evidence on lengthened partials for the deltoid specifically is limited. The practical approach: use full range of motion as the primary technique, and experiment with cable lengthened-partial sets as an accessory variation — the constant tension of the cable at the bottom position makes it more suited to this application than dumbbells.
Seated vs Standing: The Stability Trade-Off
Seated lateral raises force the deltoid to work without any lower body assistance. Standing lateral raises allow a slight controlled hip drive that lets trainees use marginally heavier loads while maintaining technique. For most hypertrophy goals, seated strict reps in the 12–20 rep range produce the most consistent medial deltoid stimulus. Standing variations are appropriate when heavier loading is the specific goal or when a slight controlled swing is used intentionally as a drop set technique after strict reps reach failure.
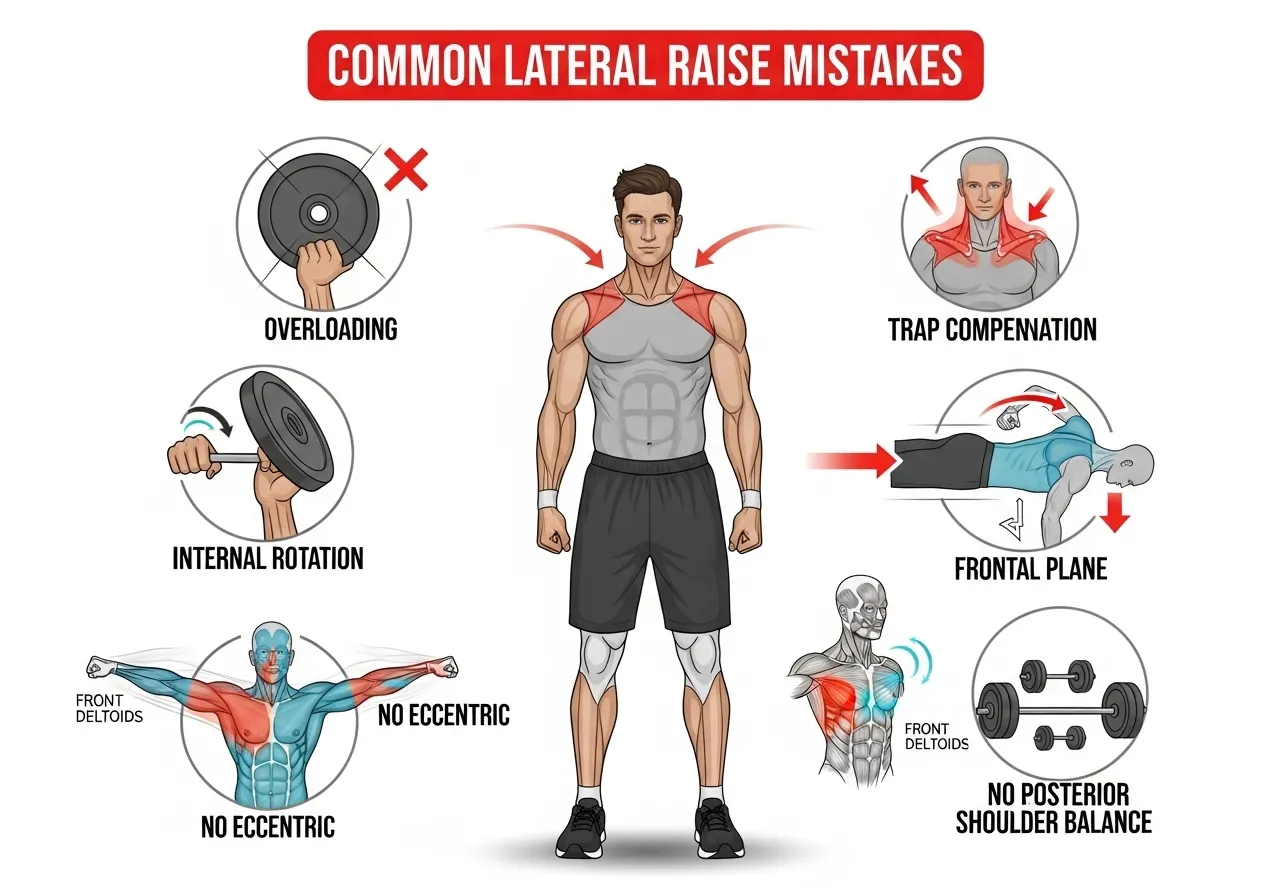
5 Lateral Raise Mistakes That Build Traps Instead of Delts
Mistake 1: Going Too Heavy
The most universal lateral raise mistake. Heavy loads force the upper trapezius to take over the lift, the lower back to lean in for momentum, and the shoulder to shrug rather than abduct purely. The medial deltoid — being the small muscle it is — cannot generate sufficient force to control heavy loading through the full range without these compensations.
The diagnostic: if you can feel your upper trap working hard during lateral raises, the weight is too heavy for strict medial deltoid training. The trap is compensating. Reduce load until the shoulder can abduct through the full range without shrugging, and feel the burn specifically in the side of the shoulder.
Mistake 2: Internal Rotation (The Pinky-Up Cue)
As the EMG research shows, internal rotation during the lateral raise shifts activation toward the posterior deltoid and upper trapezius — while increasing supraspinatus impingement risk under the acromion. The “pinky up” cue — still widely taught — is biomechanically counterproductive for medial deltoid development and potentially harmful for shoulder health when performed under load over high repetition counts.
Replace it with the neutral or slight external rotation position (thumb forward or slightly upward) and feel the difference in medial deltoid activation immediately.
Mistake 3: Raising in the Frontal Plane Rather Than the Scapular Plane
Pure frontal plane abduction (arms directly to the sides at 90° to the torso) creates greater shoulder impingement risk than scapular plane abduction (arms approximately 30° forward of true lateral). The shoulder’s natural abduction path follows the scapular plane — forcing the arms into pure frontal plane can irritate the rotator cuff over time.
Mistake 4: Not Controlling the Eccentric
Dropping the weight after each rep removes the eccentric stimulus that drives significant muscle damage and repair-based hypertrophy. Three seconds down on every rep produces dramatically better results at the same load and rep count — at the cost of feeling harder, which is precisely the point.
Mistake 5: Only Training Lateral Raises in Isolation From Shoulder Balance Work
High lateral raise volume without corresponding posterior shoulder work (face pulls, rear delt flies, external rotation) creates an anterior-medial shoulder imbalance — strong medial head, undertrained posterior cuff. For every set of lateral raises, include a set of posterior shoulder work. The face pull is the most efficient complement. See also: face pull guide for the complementary posterior shoulder programming that should accompany lateral raise volume.
The 8-Week Lateral Raise Programme
This programme runs two shoulder sessions per week. Each session includes both lateral raises and posterior shoulder work — maintaining the balance the face pull research supports.
📅 Phase 1 — Weeks 1–2: Technique Reset
Session A: Seated DB lateral raise 4×15 (strict, neutral rotation, 3-sec eccentric) | Face pull 3×15
Session B: Standing DB lateral raise 4×12 | Rear delt fly 4×15 | Face pull 2×20
Focus: Add one set per session; note whether trap fatigue or shoulder fatigue comes first
📅 Phase 3 — Weeks 5–6: Intensity + Drop Sets
Session A: Seated DB lateral raise 4×10 (heavier, still strict) + 1 drop set to failure | Face pull 3×15
Session B: Cable lateral raise 4×12 | Standing DB lateral raise 3×15 | Rear delt cable fly 3×15
Focus: First drop set — strip 40% of weight and continue to failure immediately; medial deltoid should be fully fatigued
📅 Phase 4 — Weeks 7–8: Peak + Benchmark
Session A + B: Full programme from Phase 3 with load increase where possible
Week 8 Benchmark: Retest seated lateral raise strict 15RM vs Phase 1 starting load. A 20–30% load increase at the same rep count and technique standard is a typical 8-week outcome. More important: check shoulder width in a front-facing mirror — medial deltoid development is the most visually obvious shoulder adaptation.
Focus: Establish the dual-session structure permanently — medial deltoid requires consistent direct volume to maintain and grow
Frequently Asked Questions About the Lateral Raise
How many lateral raises should I do per week?
Research on medial deltoid development suggests 12–20 direct sets per week distributed across 2–3 sessions. A practical starting structure: 4–5 sets of lateral raises at each of two shoulder sessions per week (8–10 sets total), building to 15–20 sets over 8–12 weeks as the shoulder adapts. The medial deltoid recovers quickly — twice-weekly direct training is both sufficient and sustainable.
Should I use dumbbells or a cable machine?
Both produce equivalent hypertrophy when volume and proximity to failure are matched — the research is clear on this. Choose based on availability and feel. If you have access to a low-pulley cable, the constant tension profile provides a different sensation that some trainees find more productive. If only dumbbells are available, they are equally effective. Rotating between both across training blocks provides variety without compromising outcomes.
Why do I feel lateral raises in my neck more than my shoulder?
Upper trapezius dominance — the most common lateral raise compensation. Three causes: load is too heavy, internal rotation position is driving upper trap recruitment, or the shoulder lacks the stability to maintain abduction without the trap assisting. Reduce weight by 30–40%, switch to neutral rotation (thumb forward), and slow the eccentric to 3 seconds. Most trainees feel the shift to the medial deltoid within the same session.
Can I go heavy on lateral raises for strength development?
Heavier loading (6–10 reps) is possible on lateral raises and produces strength gains alongside hypertrophy. The technical requirement is the same — neutral rotation, scapular plane, no shrugging. Heavier lateral raises typically involve a slight forward torso lean and a more controlled cheat on the concentric, allowing the muscle to work hard in the lengthened position even when the concentric requires some body momentum. See also: dumbbell training guide for programming lateral raises within a complete dumbbell shoulder workout.
Is the seated lateral raise better than the standing version?
The seated lateral raise eliminates lower body momentum and forces the deltoid to do all the work — making it more demanding per rep at the same load. For strict hypertrophy work, seated is preferable. For heavier loading where a slight controlled hip drive aids the initiation of the lift, standing allows slightly more weight while still producing high medial deltoid stimulus. Both are valid; the seated version is stricter and the standing version allows heavier absolute loads.
The trap bar deadlift carries a stigma in serious strength training communities. It is described as the easier deadlift, the beginner deadlift, the deadlift for people who cannot do a real deadlift. The perception is that its reduced range of motion and more upright torso represent a shortcut around the technical and physical demands of…
The good morning is one of the most effective posterior chain exercises in existence. It is also one of the most avoided. The name sounds casual. The movement is not. A barbell loaded across the upper back while the torso hinges forward to near-parallel creates a tremendous demand on the spinal erectors, hamstrings, and glutes…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. Why the Front Squat Is the Smarter Squat for hack squat…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only and does not replace professional medical advice. If you have any pre-existing shoulder, neck, or rotator cuff conditions, please consult a qualified healthcare professional before beginning any overhead pressing program. The overhead press guide — driving a barbell or dumbbell from shoulder height…
Back-Dominant pull-up mastery programme Blueprint This framework targets maximal back growth with safe shoulder mechanics. It builds pulling strength and total stability. Key principles:– Depress and retract the scapula before pulling.– Pull elbows toward ribs, not behind the torso.– Maintain a slight hollow body for core tension.– Progress volume and intensity in planned waves.– Track…
The Zercher squat looks uncomfortable. It is. That discomfort is also precisely what makes it effective. Named after Ed Zercher, a strongman from the 1930s who reportedly squatted this way because he lacked a squat rack, the Zercher squat holds the barbell in the crease of the elbows rather than on the back or front…