Calf and Achilles Flexibility Guide: The Research on Tight Calves, What They Limit, and How to Resolve It
Calf tightness is one of the most widespread and most underaddressed mobility restrictions in recreational athletes. Most trainees know their calves are tight. Few understand specifically what that tightness limits or how to resolve it systematically.
Restricted calf flexibility means restricted ankle dorsiflexion: the ability to bring the foot toward the shin during loaded movement. Every squat, lunge, step, and running stride depends on adequate dorsiflexion range. When that range is restricted, the body compensates upstream at the knee, the hip, and the lumbar spine.
This guide covers the anatomy of the calf complex, what the research shows about calf stretching and dorsiflexion range of motion, how calf tightness produces compensations in the squat and running gait, the most effective stretching methods, and a 6-week calf and Achilles flexibility protocol.
Gastrocnemius vs Soleus: Two Muscles That Require Different Approaches
The Two-Joint Gastrocnemius
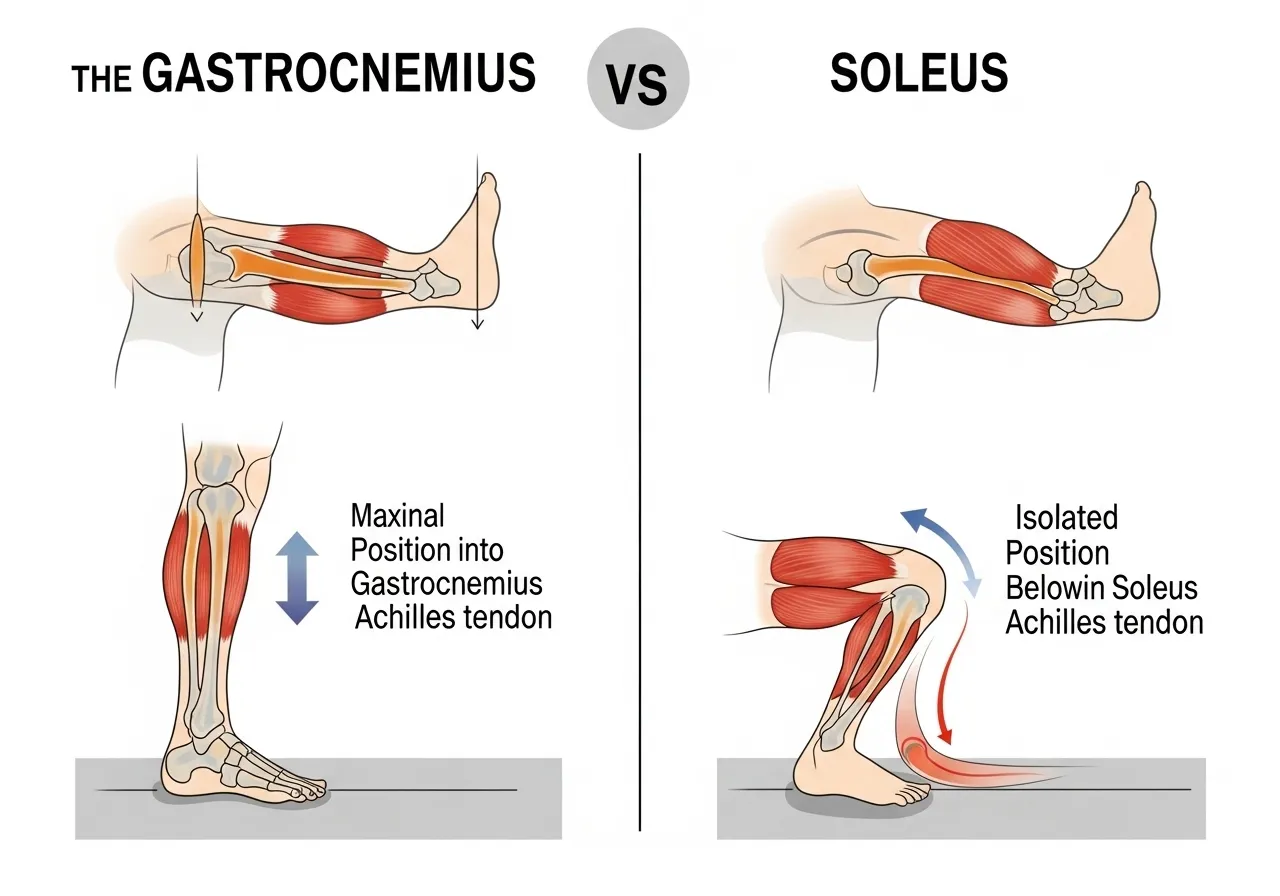
The gastrocnemius originates above the knee on the posterior femoral condyles and inserts into the calcaneus via the Achilles tendon. Because it crosses the knee joint, its flexibility is knee-position dependent. When the knee is straight, the gastrocnemius is at its full length and limits dorsiflexion maximally. When the knee is bent, the gastrocnemius becomes slack, its contribution to dorsiflexion restriction decreases, and the soleus becomes the primary limiting factor.
This anatomical distinction is why the same person can squat with adequate depth in a deep knee bend position but cannot dorsiflex adequately during walking or running, where the knee is more extended during the stance phase. The gastrocnemius is the primary culprit in standing calf tightness; the soleus is the primary culprit in flexed-knee tightness.
The Single-Joint Soleus
The soleus originates on the posterior tibia and fibula and inserts alongside the gastrocnemius into the Achilles tendon. Because it does not cross the knee, its length does not change with knee position. A tight soleus restricts dorsiflexion regardless of knee angle.
The soleus is the muscle most relevant to squat depth. When assessing calf flexibility for squat performance, a bent-knee lunge test places the stretching demand primarily on the soleus. If dorsiflexion remains restricted with the knee bent, soleus flexibility is the primary limiting factor. If the restriction resolves with knee flexion, the gastrocnemius is the primary target for stretching.
The Achilles Tendon Component
The Achilles tendon, the combined insertion of gastrocnemius and soleus, has limited extensibility as a tendon rather than a muscle. Tendons do not stretch in the same way muscles do. Tendon-targeted interventions focus on load-based adaptation rather than passive lengthening. Heavy calf raises, specifically eccentric heel drops performed at the edge of a step, are the primary tool for Achilles tendon adaptation and injury prevention, not stretching.
When dorsiflexion restriction persists despite consistent calf stretching and does not respond to either gastrocnemius or soleus-specific stretching protocols, the restriction is likely in the joint capsule or tendon rather than in the muscle belly. This situation warrants assessment before continuing to load the restriction. The ankle dorsiflexion restriction and its effects on squat mechanics are covered in detail in the ankle mobility guide.
Understanding which component is responsible for the restriction, muscle, tendon, or joint, before investing weeks in the wrong approach saves significant time. A trainee whose restriction is primarily in the talocrural joint capsule will not improve meaningfully with calf stretching. A trainee whose restriction is primarily soleus shortness will not improve with gastrocnemius-only stretching. This differentiation step, performed once at the start before committing to the full protocol, ensures that the right tools are always applied to the right tissue from the very start of the programme.
Does Calf Stretching Actually Increase Dorsiflexion Range of Motion?
The Systematic Review Evidence
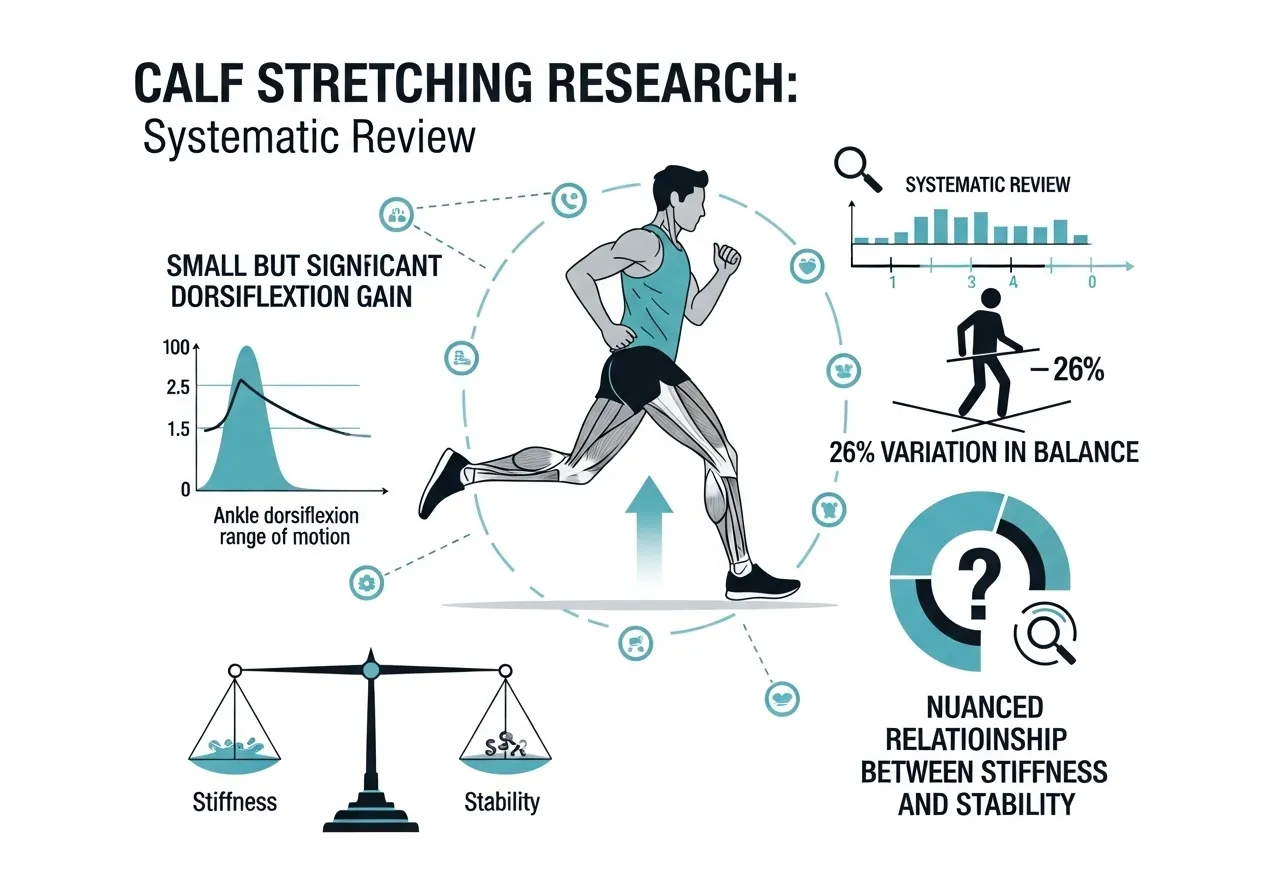
A systematic review with meta-analysis determining the effect of static calf muscle stretching on ankle joint dorsiflexion range of motion found that calf muscle stretching provides a small but statistically significant increase in ankle dorsiflexion range of motion, while acknowledging that whether this change is clinically important remains unclear, and noting that calf muscle tightness and reduced ankle dorsiflexion are related to a number of lower limb disorders including Achilles tendinitis and plantar fasciitis, making calf stretching commonly prescribed for these conditions.
Calf stretching produces statistically significant dorsiflexion range improvements, but the magnitude is modest. Stretching alone is insufficient for significant long-term dorsiflexion gains. Combining stretching with mobility drills, joint mobilisation, and loaded calf work produces superior outcomes to stretching alone.
Calf Tightness in Runners: The Trigger Point Evidence
A study examining calf tightness and ankle dorsiflexion in long-distance runners found that runners exhibit greater calf tightness and reduced ankle dorsiflexion range compared to non-runners, with research showing a 26% variation in ankle dorsiflexion range between runners and non-runners, with runners showing more restricted dorsiflexion due to calf tightness, and with overuse of the calf muscles leading to trigger point development that further restricts flexibility and contributes to injury predisposition in this population.
Runners develop greater calf tightness than non-runners despite training their calves extensively. High training volume without adequate flexibility maintenance creates progressive restriction that eventually limits performance and increases injury risk.
Calf Flexibility and Balance Control
A study examining relationships between calf muscle lengths and static and dynamic balance control found that soleus and gastrocnemius muscle flexibility as estimated by ankle dorsiflexion influenced the postural balance tests used, with less calf muscle flexibility potentially improving ankle stiffness and consequently ankle stability, reflecting better performance on balance tests, suggesting that the relationship between calf flexibility and function is more nuanced than simply more flexibility equalling better performance.
Moderate calf stiffness provides ankle stability benefits for balance. The goal is not maximum flexibility but optimal range with adequate stiffness for the demands of the sport or activity. Excessive calf flexibility can reduce ankle stability in sports requiring rapid direction changes.
What Tight Calves Actually Limit: The Compensations That Develop
The Squat: Heel Rise and Knee Cave
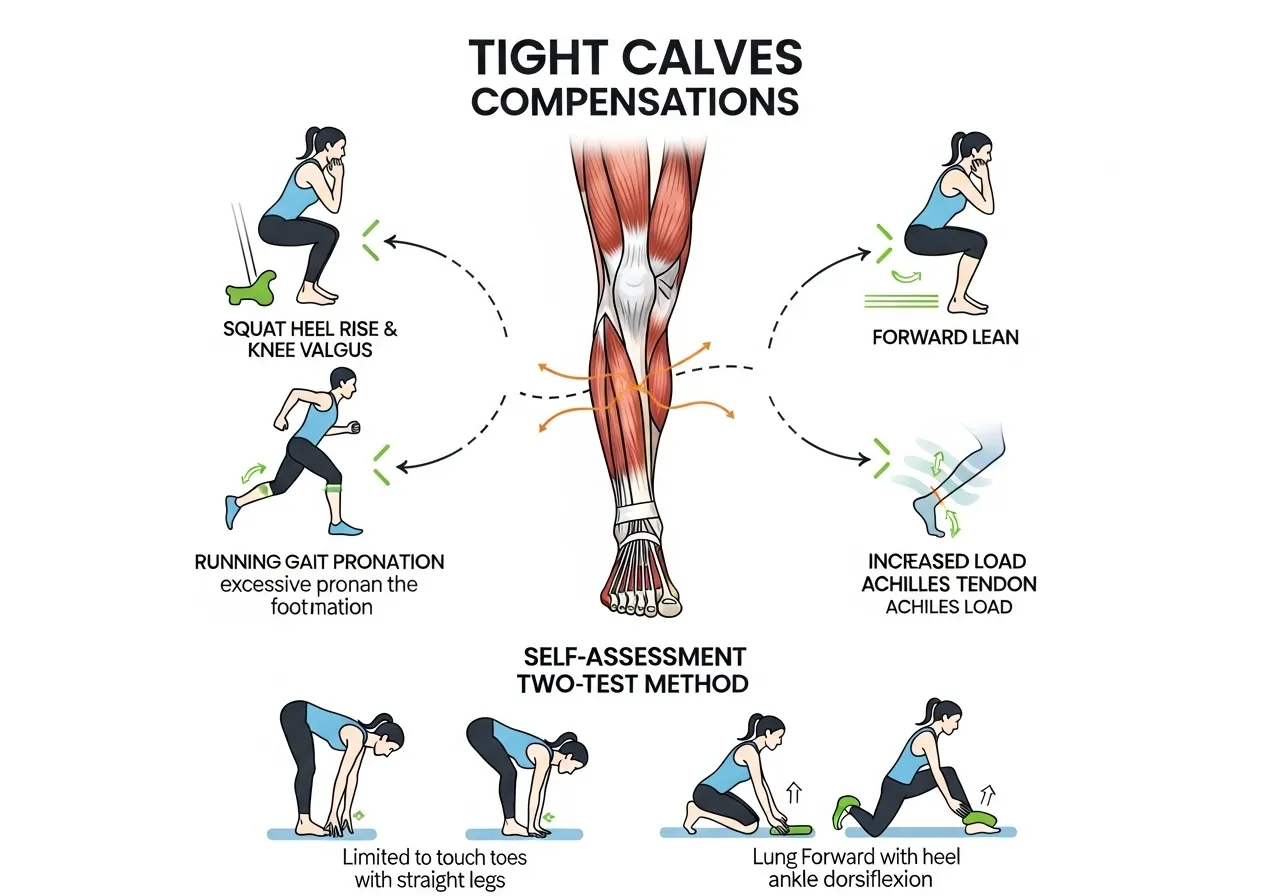
The most common compensation for restricted calf flexibility during squatting is heel rise: the heels lift off the floor to allow the body to descend without adequate ankle dorsiflexion. Heel rise shifts the body weight forward onto the toes, changes the torso angle, and increases anterior knee stress.
When heel rise is prevented, as in a flat-footed squat, the compensation shifts to the knee: the knees collapse inward (valgus) to allow the body to descend without the full dorsiflexion that a straight-ahead knee position would require. This knee valgus compensation under squat load is a significant injury risk factor for the patellofemoral joint and medial knee structures.
A third compensation in the squat is forward trunk lean. When the ankle cannot dorsiflex adequately, the hip flexes more to maintain balance, pulling the torso forward. This forward lean is often attributed to hip mobility or flexibility and treated with hip work, when the actual limiting factor is at the ankle. The evidence on stretching dosage and how long to hold stretches for genuine flexibility change is covered in the stretching for flexibility guide.
Running Gait: Ground Contact Time and Propulsion
During running, the ankle must dorsiflex during the stance phase as the body moves forward over the planted foot. Restricted calf flexibility limits this dorsiflexion, forcing compensatory internal tibial rotation and pronation that increases stress on the Achilles tendon, plantar fascia, and medial knee.
Restricted dorsiflexion also reduces the loading of the calf’s elastic energy storage during stance. The gastrocnemius and soleus store elastic energy in the Achilles tendon during the dorsiflexion phase and release it during toe-off. Restricted dorsiflexion reduces the loading phase, reducing the elastic energy available for propulsion. Runners with tight calves are effectively running with less energy return from the Achilles spring mechanism than their range of motion would allow.
The compensatory patterns from calf tightness extend beyond the ankle and calf. When the ankle cannot dorsiflex adequately, the knee and hip must produce additional work to achieve forward progression. This upstream demand increases metabolic cost per stride and accelerates fatigue in the knee extensors and hip flexors, muscles that are not designed to bear the extra load. Runners with unexplained knee fatigue or hip flexor tightness that does not resolve with direct hip work often find that addressing calf flexibility resolves these secondary complaints without any treatment directed at the hip or knee specifically.
Identifying Your Primary Restriction
Two self-tests identify whether the gastrocnemius or soleus is the primary limiting factor:
- Standing calf stretch (knee straight): Face a wall. Place the foot being tested 30 to 40 cm from the wall. Keep the knee straight and drive the heel into the floor while leaning the shin toward the wall. This stretches the gastrocnemius primarily. The distance the foot must be from the wall to feel the stretch indicates gastrocnemius flexibility.
- Bent-knee lunge test (knee bent): Kneel on one knee with the front foot flat. Drive the front knee forward over the toes while keeping the heel flat on the floor. This stretches the soleus primarily. If this is more restricted than the standing test, soleus is the primary target.
The 6 Most Effective Calf and Achilles Flexibility Exercises
🦵 1. Straight-Leg Calf Stretch (Gastrocnemius Target)
Target: Gastrocnemius, Achilles tendon
How: Stand facing a wall with hands flat against it. Step one foot back 60 to 80 cm. Keep the rear knee straight and the rear heel flat on the floor. Lean into the wall until the stretch is felt in the back of the lower leg. Hold 30 to 45 seconds.
Key point: The heel must remain flat on the floor. Lifting the heel means the gastrocnemius is not being adequately stretched. Move the foot further from the wall if the heel rises under the stretch.
🦵 2. Bent-Knee Calf Stretch (Soleus Target)
Target: Soleus, deep calf, squat position preparation
How: Same starting position as the straight-leg stretch but with the rear knee bent 20 to 30 degrees. The bent knee takes the gastrocnemius slack and targets the soleus specifically. Hold 30 to 45 seconds. This is the most relevant calf stretch for squat depth development.
Key point: The stretch feels lower in the calf and closer to the ankle than the gastrocnemius stretch. If there is no sensation of stretch with the knee bent, move the foot closer to the wall and increase the knee bend.
🦵 3. Incline Board or Step Stretch
Target: Gastrocnemius, Achilles under sustained load
How: Stand with the toes on a slant board inclined at 15 to 25 degrees or on the edge of a step with heels hanging off. Allow gravity to stretch the calf by descending the heel below the toes. Hold for 30 to 60 seconds per side.
Key point: The incline board version provides a passive, gravity-assisted stretch that is particularly effective for sustained holds. Adding a slight bend in the knee shifts the target toward the soleus.
🦵 4. Eccentric Heel Drop
Target: Achilles tendon adaptation, gastrocnemius and soleus eccentric strength
How: Stand on the edge of a step on the balls of both feet. Rise onto the toes with both feet, then transfer to one foot only. Lower the heel slowly below the step edge over 3 to 5 seconds. Return to two-foot rise and repeat. Perform 3 sets of 15 reps per side.
Key point: This is not purely a stretching exercise. It is the primary Achilles tendon strengthening and adaptation exercise. Eccentric heel drops have the strongest evidence base for Achilles tendinopathy rehabilitation. The bent-knee variation (knee bent 30 degrees throughout) targets the soleus and Achilles below the musculotendinous junction.
🦵 5. Wall Ankle Dorsiflexion Mobilisation
Target: Ankle joint dorsiflexion, talocrural joint mobility
How: Stand facing a wall with the foot being mobilised 5 to 10 cm from the wall. Drive the knee forward over the second toe to touch the wall. Keep the heel flat. If the knee can touch the wall, move the foot further away. Test and work at the distance where heel stay flat but the knee barely reaches the wall.
Key point: This test and mobilisation drill addresses ankle joint mobility, not just muscle length. If dorsiflexion remains restricted despite consistent muscle stretching, this drill targets the joint capsule component that muscle stretching cannot affect.
🦵 6. Foam Roll Calf Release
Target: Calf tissue quality, trigger points, pre-stretch preparation
How: Sit on the floor with the foam roller under the calf. Use the arms to lift the hips and roll slowly from the ankle to just below the knee. Pause on any tender points for 20 to 30 seconds. Rotate the leg internally and externally to address different portions of the calf.
Key point: Foam rolling before stretching reduces the neural resistance to stretching and improves the immediate effect of the subsequent static or dynamic work. The research on foam rolling and its mechanism is covered in the foam rolling guide.
Why Does Calf Tightness Keep Returning Despite Regular Stretching?
The Training Volume Problem
Runners and athletes who train high volumes repeatedly contract the calf musculature hundreds of thousands of times per week. Each contraction shortens the muscle temporarily. Without adequate recovery and flexibility work between sessions, the accumulated shortening effect exceeds what intermittent stretching can reverse.
For high-volume athletes, stretching frequency needs to match training frequency. Stretching the calves twice a week while running 50 km per week is insufficient to maintain flexibility. The minimum effective dose for runners with persistent calf tightness is calf stretching after every run session, not every other day or twice weekly.
The Neurological Component
Muscle tightness is not always structural. Neurological tone, the background activation level of the muscle maintained by the nervous system, creates tightness that does not change with passive stretching because the muscle is not structurally shortened. The nervous system is maintaining it in a heightened state of readiness due to overuse, fatigue, or protective responses following minor injury.
Trigger points, localised areas of heightened muscle activity within the calf, create this neurological tightness. Foam rolling, dry needling, and massage specifically address trigger points. Standard static stretching does not resolve trigger point tension because it does not address the neurological source. Trainees who stretch consistently without improvement usually have significant trigger point activity rather than, or in addition to, structural muscle shortness.
Joint Mobility vs Muscle Flexibility
A portion of dorsiflexion restriction originates in the ankle joint itself, specifically in the talocrural joint capsule and any posterior joint impingement. These structural restrictions do not respond to muscle stretching because the limiting tissue is not muscle. Joint mobilisation work, specifically the wall ankle mobilisation drill described above, addresses this component.
Trainees who have stretched their calves consistently for months without measurable dorsiflexion improvement likely have a significant joint component to their restriction. Adding the wall ankle mobilisation drill 5 to 10 minutes before every stretching session, particularly on training days and before lower body gym work, produces dorsiflexion gains that stretching alone consistently fails to achieve. The complete framework for ankle mobility including joint mobilisation and how it relates to squatting and running performance is in the ankle mobility guide.
6-Week Calf and Achilles Flexibility Protocol
📅 Weeks 1 to 2: Tissue Quality and Assessment
- Foam roll calves: 2 minutes per side, daily
- Straight-leg calf stretch: 3 sets of 45 seconds per side, twice daily
- Bent-knee calf stretch: 3 sets of 45 seconds per side, twice daily
- Wall ankle mobilisation: 3 sets of 10 knee drives per side, daily
- Assess: measure finger-to-wall distance in the wall ankle mobilisation at start and end of Week 2
Focus: Establish the baseline and begin tissue quality improvements. Twice-daily stretching in Phase 1 is intensive but temporary, designed to produce rapid initial change.
📅 Weeks 3 to 4: Loaded Calf Work and Mobility Integration
- Continue stretching: reduce to once daily (before training or in the evening)
- Add eccentric heel drops: 3 sets of 15 per side, 3 days per week
- Incline board stretch: 3 sets of 60 seconds per side, after training sessions
- Integrate wall ankle mobilisation into squat or running warmup
Focus: Add tendon loading alongside flexibility work. Eccentric heel drops produce Achilles adaptation that passive stretching alone cannot achieve.
📅 Weeks 5 to 6: Maintenance Standard and Performance Integration
- Calf stretching: once daily as permanent habit
- Eccentric heel drops: 3 sets of 15 per side, twice weekly ongoing
- Reassess wall ankle mobilisation distance versus Week 1 baseline
- Test squat depth and running mechanics for compensation reduction
Focus: Establish the long-term maintenance standard. The daily stretching and twice-weekly eccentric work becomes the permanent calf and Achilles maintenance programme beyond Week 6.
Frequently Asked Questions About Calf and Achilles Flexibility
How long does it take to increase calf flexibility?
With the twice-daily stretching protocol in Weeks 1 to 2, measurable dorsiflexion improvements typically appear within 2 to 3 weeks. The wall ankle mobilisation test provides an objective measurement: most trainees gain 1 to 2 cm of additional reach within the first four weeks of consistent work combining stretching, foam rolling, and joint mobilisation.
Significant functional improvement, enough to noticeably change squat depth or reduce running compensations, typically requires 6 to 8 weeks of consistent daily work. Calf flexibility restricted for years requires sustained consistent effort rather than short intensive blocks.
Should I stretch before or after training?
Static calf stretching before training may temporarily reduce calf muscle power and tendon stiffness, which is counterproductive for activities requiring calf strength and reactivity such as jumping, sprinting, and plyometric training. The standard recommendation is dynamic calf mobilisation (ankle circles, calf raises, walking lunges) before training and static stretching after.
The wall ankle mobilisation drill is an exception: it can be performed before training because it targets joint mobility rather than muscle length and does not reduce calf power output. Including 2 to 3 minutes of wall ankle mobilisation in any lower body training warmup improves ankle dorsiflexion for the session without the performance reduction associated with static pre-training stretching.
What is the difference between calf tightness and Achilles tendinopathy?
Calf muscle tightness is a flexibility restriction in the gastrocnemius or soleus muscle belly. Achilles tendinopathy is a degenerative or overuse condition of the tendon itself, characterised by localised pain, stiffness, and thickening at the tendon. They often co-exist because restricted calf flexibility increases tensile load on the Achilles tendon during activity.
The treatments differ. Muscle tightness responds primarily to stretching and soft tissue work. Tendinopathy responds primarily to progressive tendon loading through eccentric exercises, specifically eccentric heel drops, combined with load management. Treating tendinopathy with stretching alone produces limited results because the tendon, not the muscle, is the pathological tissue. The stretching guidance in this guide applies to muscle tightness. Active Achilles tendinopathy requires a graded loading programme rather than a flexibility programme.
How do I know if my calf tightness is affecting my squat?
The simplest test is to compare squat depth with heels flat on the floor versus heels elevated on plates or a wedge. If adding 2 to 3 cm of heel elevation significantly improves squat depth or removes the compensations you observe (heel rise, forward lean, knee cave), restricted ankle dorsiflexion is a primary limiting factor in your squat.
A more specific test is the weight-bearing lunge test: stand 10 cm from a wall and drive the knee forward to touch the wall while keeping the heel flat. If your knee cannot reach the wall at 10 cm distance, your dorsiflexion is restricted relative to the minimum needed for squat depth. For most trainees, 12 to 15 cm of knee-to-wall distance indicates adequate dorsiflexion for comfortable squat mechanics. The full squat depth and ankle dorsiflexion assessment is detailed in the ankle mobility guide.
Addressing calf tightness as a deliberate training priority for 6 to 8 weeks, rather than a casual afterthought, produces the most measurable changes. Daily stretching, regular joint mobilisation work, and progressive Achilles loading combine to produce cumulative dorsiflexion improvements that occasional stretching alone cannot achieve.
- Gastrocnemius and soleus require different stretching positions. Straight-leg stretches target the gastrocnemius. Bent-knee stretches target the soleus, which is the primary limiting factor for squat depth.
- Calf stretching produces small but significant dorsiflexion improvements. Combining stretching with joint mobilisation and eccentric loading produces superior outcomes to stretching alone.
- Runners develop greater calf tightness than non-runners despite training volume. Post-run stretching frequency must match training frequency to prevent progressive restriction.
- Trigger point activity creates neurological tightness that static stretching does not resolve. Foam rolling and trigger point work must precede stretching for maximum effectiveness.
- Eccentric heel drops are the primary Achilles tendon adaptation exercise. They develop tendon load capacity that passive stretching cannot produce.