⚠️ Health & Fitness Disclaimer This article is for general educational and informational purposes only. It does not replace professional medical or fitness advice. If you have any pre-existing condition, injury, or chronic pain — please consult a qualified healthcare professional or certified personal trainer before starting or modifying any foam rolling basics or mobility program.
Foam rolling has gone from a niche physical therapy tool to a standard fixture in gyms worldwide — yet the evidence behind it is more nuanced than most fitness content suggests.
Does it work? Yes — for some outcomes, under specific conditions.
Does it do everything its marketing claims? No — the research tells a more complicated story.
This guide covers what foam rolling actually does according to the evidence, how to apply it effectively for both warm-up and recovery, and the practical protocols that produce meaningful results.
What Foam Rolling Actually Does: The Evidence-Based Overview
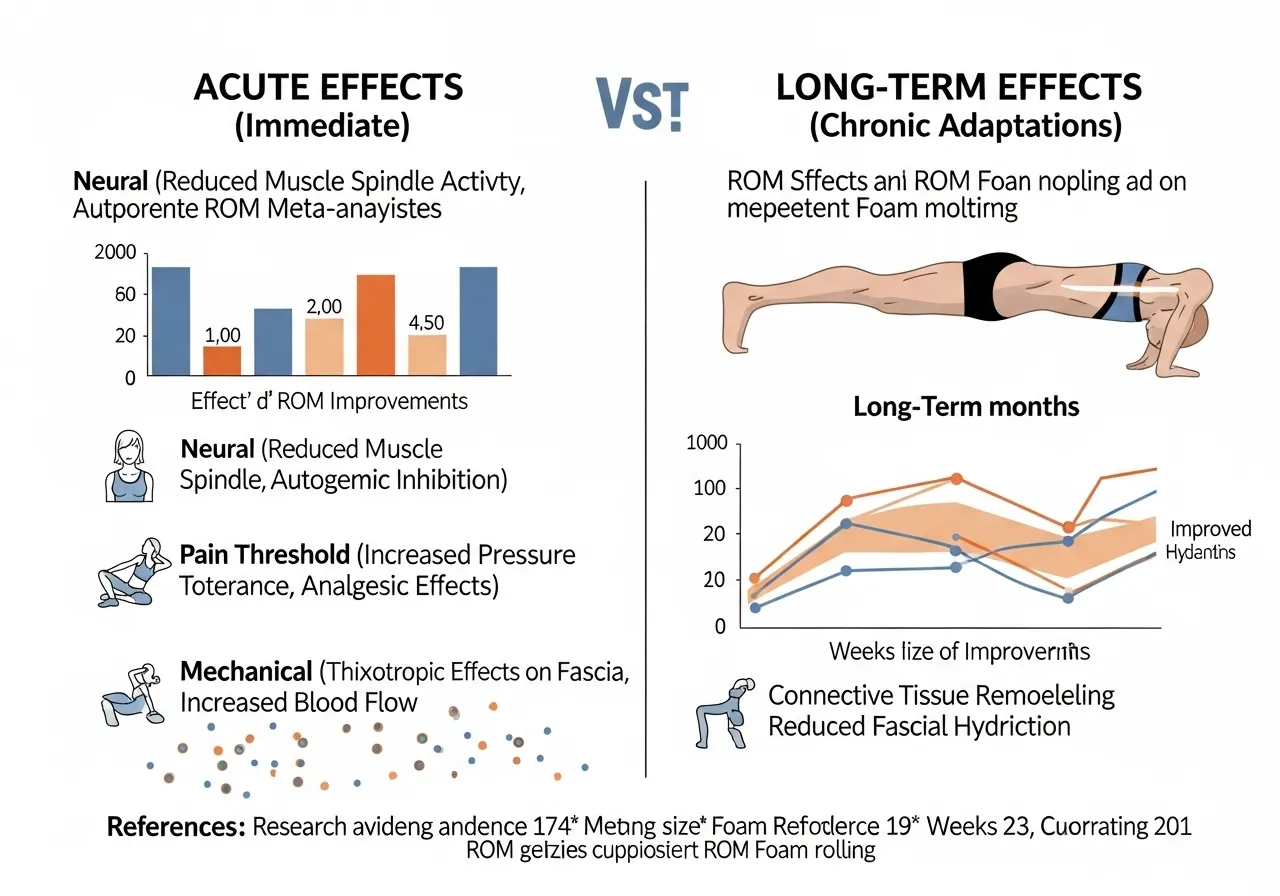
Acute vs. Long-Term Effects: A Critical Distinction
The majority of foam rolling research measures acute effects — what happens immediately after a single foam rolling session.
Acute effects that are well-supported by research include:
Increased joint range of motion (ROM) — lasting approximately 10–30 minutes after rolling
Reduced muscle soreness perception after exercise
Temporary reduction in muscle stiffness (the resistance a muscle offers to passive stretching flexibility guide)
Long-term effects from consistent foam rolling training are less extensively studied but are emerging in the literature.
The “no detrimental effects” finding is significant — unlike prolonged static stretching (which can temporarily reduce strength output), foam rolling before training does not appear to impair power, strength, or sprint performance.
This makes foam rolling a more practical pre-training mobility tool than static stretching for athletes and strength trainees who need to maintain performance capacity.
This finding carries a practical implication: pre-workout foam rolling may provide more reliable benefits than post-workout rolling for most trainees, though post-workout rolling may still help reduce perceived soreness.
How Foam Rolling Works: The Proposed Mechanisms
The exact mechanisms behind foam rolling’s effects are still being researched, but current evidence supports several contributing factors:
Neural mechanism (pain threshold modulation): Foam rolling may increase the pain pressure threshold (the minimum pressure required to produce a pain sensation) through gate control theory — pressure signals competing with pain signals at the spinal cord level, temporarily reducing perceived muscle tightness
Mechanical tissue effects: Direct pressure on the muscle-tendon unit may produce transient changes in tissue stiffness and extensibility
Blood flow increase: The compression and release pattern may temporarily increase local blood flow to the rolled area
Fascial effects: Some researchers propose effects on the fascia (the connective tissue surrounding muscles), though the evidence for direct fascial remodeling from foam rolling is limited
The neural pain threshold mechanism currently has the strongest research support — which helps explain why the ROM effects are acute (neural changes are immediate but temporary) and why consistency over weeks is needed for lasting structural changes.
What Research Transparency Means for Your Foam Rolling Practice
The honest summary of foam rolling research is this: it works, but modestly and through mechanisms that are not yet fully understood.
The consistent finding across multiple meta-analyses — large effect sizes for acute ROM improvement, no negative effects on performance, modest recovery benefits — justifies including foam rolling in a training program.
But it does not justify the exaggerated claims common in fitness marketing: that it “breaks up scar tissue,” “releases fascia,” or “fixes” chronic tightness in a single session.
The trainees who benefit most from foam rolling tend to be those who use it consistently as part of a daily mobility practice — not those who use it intensively but occasionally.
Setting accurate expectations helps maintain the practice long enough for the research-supported benefits to accumulate over weeks and months of consistent use.
Foam Rolling and Other Recovery Modalities: How It Compares
Recovery Tool
Evidence Strength
Primary Benefit
Practical Accessibility
Foam rolling
Moderate
ROM, soreness reduction
High — inexpensive, home use
Sleep (7–9 hrs)
Very Strong
Full systemic recovery
High — no equipment
Static stretching
Strong
Flexibility, ROM
High — no equipment
Professional massage
Moderate
Soreness, ROM, relaxation
Low — cost, scheduling
Ice/contrast bathing
Moderate
Acute soreness, swelling
Moderate
Among accessible, low-cost recovery tools, foam rolling and sleep provide the best combination of evidence support and practical ease — with sleep quality consistently identified as the most important single recovery factor for athletic performance and muscle adaptation.
Duration and Frequency: What the Research Specifically Recommends
Synthesizing the available meta-analyses, the most evidence-supported foam rolling approach combines:
30–90 seconds per muscle area per session — enough for acute ROM response without excessive time investment
Daily practice over 4+ weeks — the threshold at which research shows significantly greater ROM improvements than shorter protocols
Moderate rolling speed (approximately 2–3 cm per second) — allowing sufficient pressure contact time without rushing through the tissue
Consistent targeting of the same muscle groups — random area-to-area rotation without consistent return to the same muscles may reduce cumulative adaptation
These parameters are not absolute — individual tolerance, specific training goals, and available time all appropriately influence session design.
But they represent a practical starting framework grounded in what the research specifically supports rather than gym tradition or marketing claims.
Approached this way — as a consistent daily habit rather than an occasional intensive session — foam rolling produces meaningful and lasting flexibility improvements over time. The evidence clearly supports this practice. .
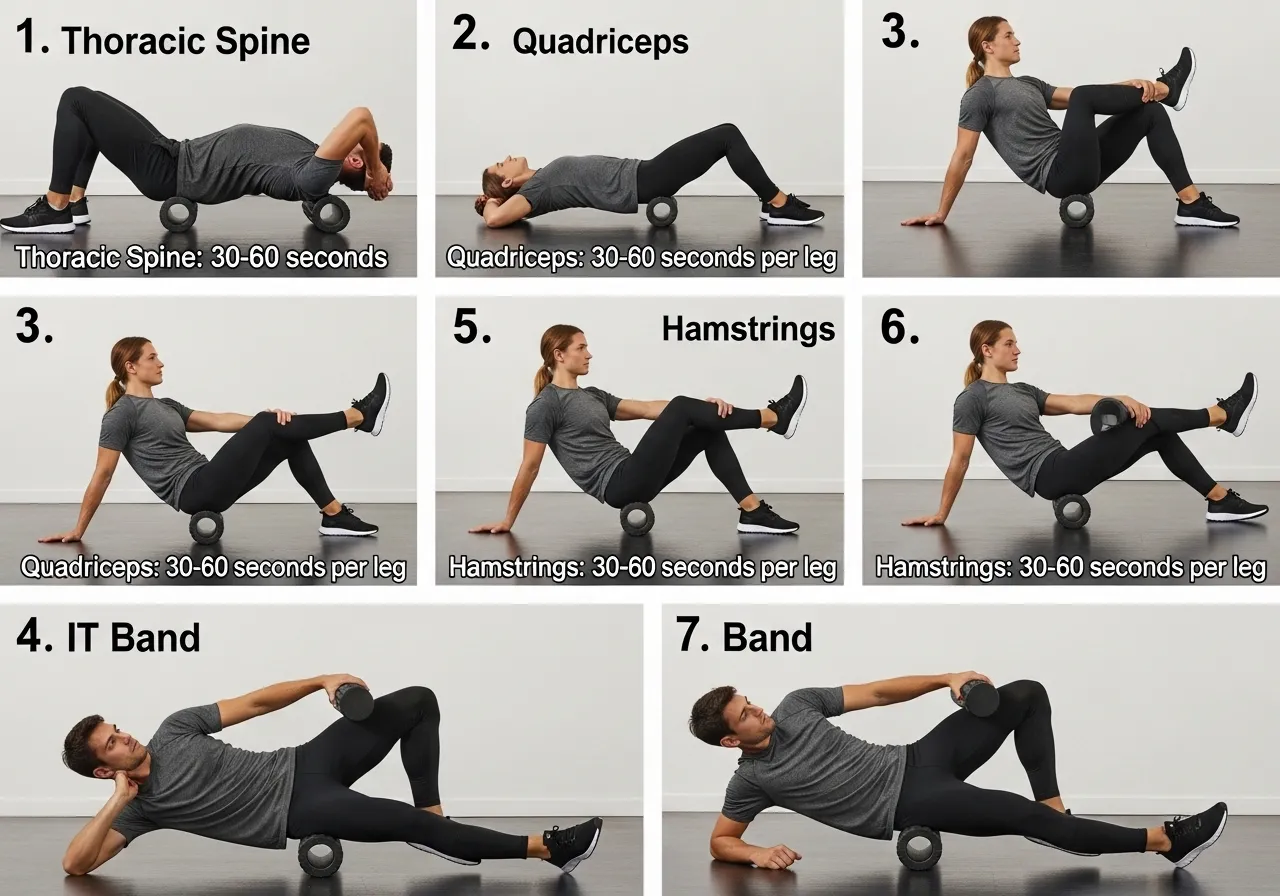
The 7 Essential Foam Rolling Techniques and Target Areas
1 — Thoracic Spine (Upper Back)
One of the most universally beneficial foam rolling applications — the thoracic spine (the 12 vertebrae of the mid-back connecting the cervical neck and lumbar lower back) is frequently stiff in desk workers and overhead athletes. (see also: lower back pain stretches)
Technique: Place the foam roller perpendicular to the spine at mid-back level. Support the head with interlaced hands. Lift the hips slightly and roll 3–5 cm up and down the thoracic region, pausing on areas of increased tension for 20–30 seconds. Duration: 60–90 seconds total across the thoracic spine
⚠️ Do not roll the lumbar (lower) spine in this position — the lack of rib cage support at the lumbar level means this position can increase lumbar stress rather than reduce it
2 — Quadriceps (Front of Thigh)
The quadriceps group — vastus lateralis, vastus medialis, rectus femoris, and vastus intermedius — is one of the most responsive muscle groups to foam rolling in terms of documented ROM improvement.
Technique: Prone (face down) position with the roller under the front of one or both thighs. Shift weight toward the outer portion (IT band side) to address the vastus lateralis, then shift inward for the inner quad. Roll from just above the knee to the hip crease. Duration: 60–90 seconds per leg Pressure guidance: Apply enough pressure to feel moderate discomfort (4–6 on a 10-point pain scale) — less than this may be insufficient stimulus; more than this is not necessary and may cause unnecessary pain
3 — Hamstrings (Back of Thigh)
Technique: Seated with the roller under the back of one thigh, hands on the floor behind you. Roll from just above the knee to the glute fold. Cross the opposite leg over the top of the working leg to increase pressure if needed. Duration: 60–90 seconds per leg
4 — IT Band and Lateral Thigh
The iliotibial band (IT band — a thick band of fascia running from the hip down the outer thigh to the knee) is a frequent rolling target for runners, cyclists, and knee pain sufferers.
Important context: the IT band is a dense fibrous structure, not a muscle — it does not “release” in the way muscles do, and the intensity of pain when rolling the IT band is not proportional to any structural change occurring.
Rolling the outer thigh (vastus lateralis) below the IT band, and the TFL (tensor fasciae latae — the muscle at the hip that connects to the IT band) above it, may be more productive than trying to forcibly compress the IT band itself.
Technique: Side-lying with the roller under the outer thigh. Support with the top foot on the floor for pressure control. Roll from just above the knee to the hip. Duration: 60 seconds per side
5 — Calves (Gastrocnemius and Soleus)
Technique: Seated with the roller under one calf, other leg crossed over the top. Roll from the ankle to just below the knee. Rotate the foot inward and outward to address different portions of the calf. Duration: 60–90 seconds per leg Note: Research shows foam rolling has limited effect on ankle dorsiflexion ROM specifically — calf rolling may be more effective for reducing calf soreness than for improving ankle mobility
6 — Lats and Upper Back
Technique: Side-lying with the roller under the armpit area. Arm extended overhead. Roll from the armpit down to the lower ribcage area, targeting the latissimus dorsi (the broad back muscle connecting the lower back to the upper arm). Duration: 60 seconds per side — especially useful before pull-up and row sessions
7 — Glutes and Piriformis
The piriformis (a small, deep hip muscle that can compress the sciatic nerve when tight or hypertonic) and the gluteus medius are often areas of tension that benefit from targeted rolling.
Technique: Seated on the roller, one ankle crossed over the opposite knee (figure-4 position). Shift weight toward the crossed-leg side glute. Roll in small circles or hold pressure on tender areas for 20–30 seconds. Duration: 60–90 seconds per side
⚠️ If sciatica-type pain (radiating down the leg) is present, consult a physiotherapist before applying direct pressure to the piriformis area
Foam Rolling the Feet: The Plantar Fascia Application
Rolling the plantar fascia (the thick band of connective tissue running along the sole of the foot from the heel to the toes) using a massage ball or small dense roller is a commonly used intervention for plantar fasciitis prevention and management.
The technique involves placing a lacrosse ball or golf ball under the arch of the foot while standing or seated, applying moderate pressure, and rolling in small circles or slowly along the arch.
Important note: established plantar fasciitis is a clinical condition requiring professional assessment and treatment — foam rolling the foot may provide temporary symptom relief but is not a replacement for physiotherapy evaluation if plantar heel pain is present.
Trigger Point Technique vs. Continuous Rolling
Two distinct application styles exist within foam rolling practice:
Continuous rolling: Slowly moving up and down the muscle belly — the most common technique; effective for general ROM and recovery goals
Trigger point / ischemic compression: Finding an area of localized increased tenderness and holding pressure on it for 20–30 seconds until the sensation reduces — used for addressing specific points of increased muscle tension
The trigger point approach requires finding the specific area of tension within the muscle — this technique is more time-intensive than continuous rolling but may produce greater local release in areas of concentrated tightness.
Combining both approaches — rolling continuously through the muscle first to identify tender areas, then holding pressure on the most notable points for 20–30 seconds — is a practical and comprehensive rolling session structure.
Foam Rolling for Shoulder Mobility
The posterior shoulder — specifically the posterior capsule and the infraspinatus — is frequently tight in overhead athletes, bench press-heavy trainees, and desk workers who carry the shoulders in internal rotation.
Using a lacrosse ball against a wall for posterior shoulder rolling provides targeted access that a floor-based foam roller cannot achieve:
Place the ball against the wall at shoulder height, pressing the back of the shoulder into it
Make small circles or shift the shoulder in internal and external rotation to cover the posterior capsule area
60 seconds per side — particularly useful before overhead pressing or pulling sessions
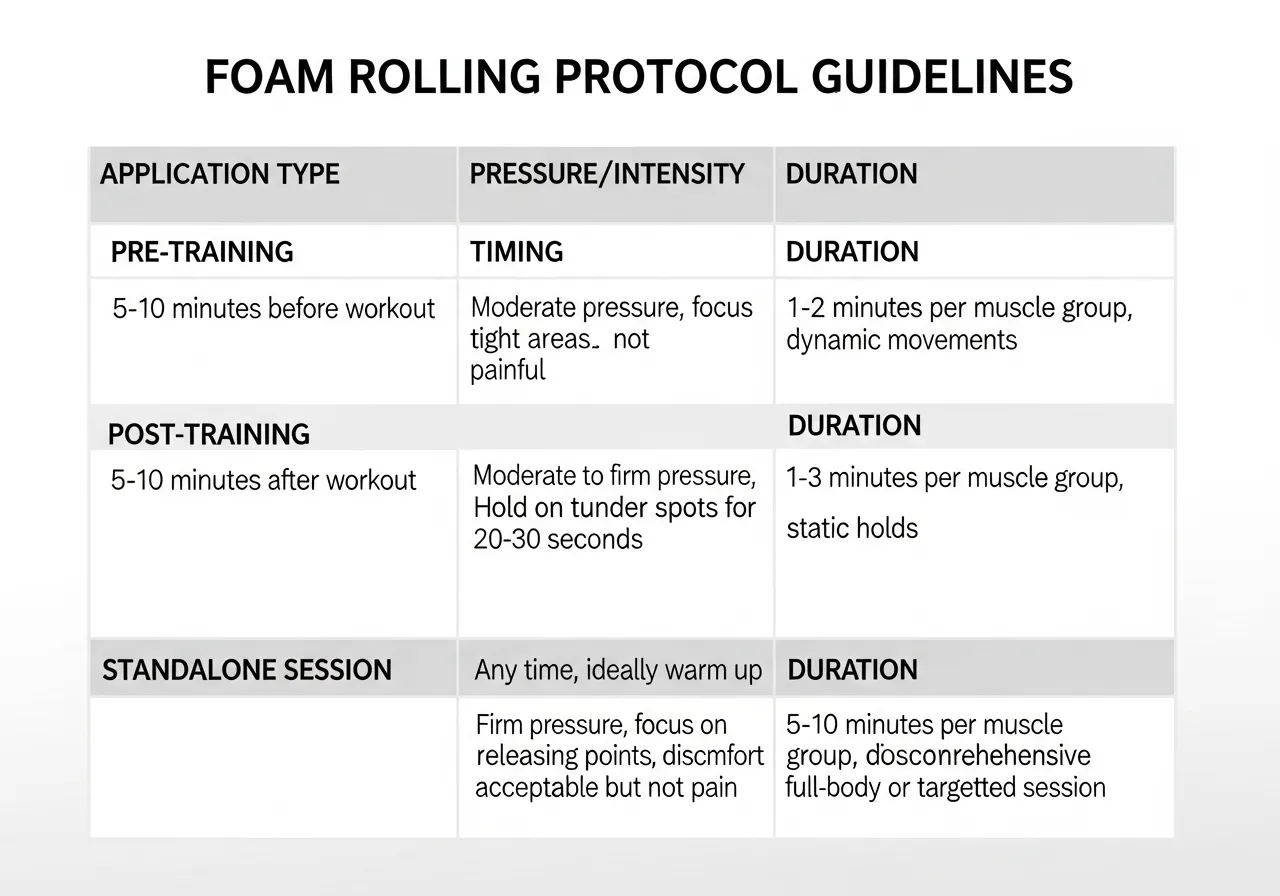
Foam Rolling Protocols: Timing, Duration, and Pressure Guidelines
Pre-Training Foam Rolling: The Warm-Up Application
Foam rolling before training is supported as an effective warm-up component — it increases ROM without the performance reduction associated with prolonged static stretching.
Optimal pre-training protocol:
Variable
Recommendation
Rationale
Duration per area
30–60 seconds
Sufficient for acute ROM response without excessive time
Rolling speed
Moderate — 2–3 cm/sec
Allows sufficient pressure contact time
Pressure intensity
Moderate (4–6/10 discomfort)
Lower pressure may be insufficient; higher unnecessary
Areas to target
Muscles to be used in the upcoming session
Session-specific rolling maximizes relevant ROM benefit
Total pre-rolling time
5–10 minutes
Practical within warm-up time constraints
Post-Training Foam Rolling: The Recovery Application
Post-training foam rolling is supported for reducing perceived muscle soreness (DOMS — delayed onset muscle soreness) over the 24–72 hours following exercise.
The magnitude of the effect on soreness perception is modest — typically a subjective reduction of 1–2 points on a 10-point scale — but many trainees find this meaningful for recovery comfort.
Variable
Recommendation
Duration per area
60–120 seconds — longer than pre-training is acceptable
Rolling speed
Slow — allow 30-second holds on tender areas
Areas to target
Muscles that were trained in the session
Total post-rolling time
5–15 minutes
Standalone Mobility Sessions
Using foam rolling as part of a dedicated daily mobility session — separate from training — is the format most likely to produce lasting flexibility improvements.
Example 15-minute daily morning mobility routine:
✅ Thoracic spine rolling — 90 seconds
✅ Quadriceps rolling — 90 seconds per leg
✅ hamstring flexibility rolling — 60 seconds per leg
✅ Glute/piriformis rolling — 60 seconds per side
✅ Static stretching of rolled areas — 30–45 sec × 2 per muscle
✅ Light dynamic movement — 5 minutes (hip circles, leg swings, shoulder rotations)
The combination of foam rolling followed immediately by static stretching may produce greater ROM improvements than either modality alone — the rolling reduces neural tone in the muscle, potentially allowing the subsequent stretch to reach a greater tissue length.
Pressure and Pain: Finding the Right Intensity
A common misconception: more pain during foam rolling means more benefit.
Current evidence does not support extreme pain (7–10/10 discomfort) as producing better outcomes than moderate pressure (4–6/10).
Practical pressure guidance:
2–3/10: Likely insufficient mechanical input for meaningful neural or mechanical change
4–6/10: Target zone — notable but not distressing discomfort; the neural pain modulation mechanism is engaged
7+/10: No additional benefit over moderate pressure; muscles may involuntarily tense in response to excessive pain, working against the goal of reduced stiffness
When Foam Rolling Is Not Enough: Seeking Professional Input
Several situations suggest that foam rolling alone is insufficient and professional guidance would produce better outcomes:
Persistent tightness in a specific area that does not improve after 6–8 weeks of consistent daily rolling — a different mechanism (joint restriction, nerve involvement, structural issue) may be present
Pain during rolling that is sharp, electrical, or radiating rather than a dull compression feeling — nerve involvement requires professional assessment
Tightness that is noticeably asymmetrical (one side significantly tighter than the other) despite equivalent treatment — unilateral tightness may reflect a compensatory pattern worth assessing
Mobility limitations that are affecting training performance or daily activities despite a consistent mobility practice
A physiotherapist, sports massage therapist, or certified mobility specialist can provide individual assessment that identifies whether a specific limitation requires targeted manual therapy, specific exercise prescription, or a different approach than self-directed foam rolling.
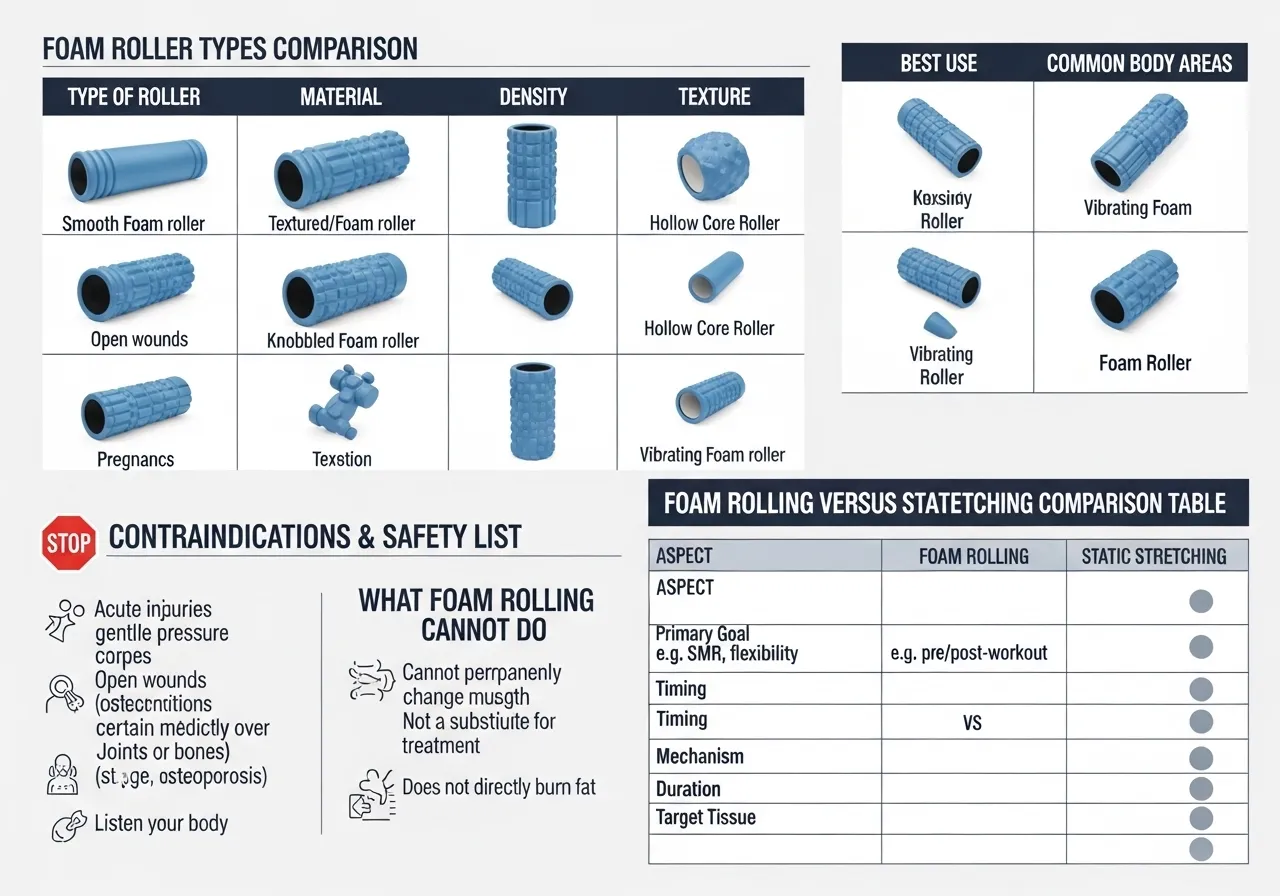
Foam Rolling Tools, Limitations, and What It Cannot Do
Choosing a Foam Roller
Type
Density/Feature
Best For
Soft smooth roller
Low density, smooth surface
Beginners, very sensitive areas, post-surgery recovery
Medium density roller
Standard density
Most trainees — practical starting point
High density / textured
Firm, with ridges/knobs
More pressure for larger, denser muscles
Vibrating foam roller
Added vibration mechanism
Greater ROM improvements than standard rolling per meta-analysis
Being accurate about limitations is important for managing expectations and avoiding disappointment:
It does not “break up adhesions”: The forces generated by a foam roller are insufficient to physically break up fascial adhesions (areas where connective tissue layers have become abnormally stuck together) — despite this claim being widely repeated in fitness content
It does not produce lasting structural changes in a single session: Acute ROM improvements fade within 20–30 minutes; structural changes require consistent practice over weeks
It is not a substitute for medical treatment: Foam rolling cannot treat disc herniations, nerve entrapments, structural joint problems, or serious muscle injuries — these require professional evaluation and treatment
IT band “release” is not occurring: The IT band’s density makes it mechanically unlikely to change from foam roller pressure — neural effects on the surrounding muscles are a more plausible mechanism
Contraindications: When NOT to Foam Roll
⚠️ Avoid foam rolling over:
→ Acute injuries (within 72 hours of significant trauma — allow initial healing first)
→ Areas with active inflammation, redness, or swelling
→ Varicose veins or blood clot risk areas
→ Directly over the lower lumbar spine (use thoracic rolling with caution extending to thoracolumbar junction)
→ Bony prominences (hip bones, knee bones, spine processes) — roll the muscle belly, not the bone
→ Areas of numbness or altered sensation — impaired feedback increases injury risk
If you have a diagnosed medical condition and are unsure whether foam rolling is appropriate, consulting your healthcare provider or physiotherapist before beginning is recommended.
Foam Rolling vs. Stretching: Complementary, Not Competing
Research comparing foam rolling and static stretching for ROM improvements shows that both produce similar acute ROM increases — but through different mechanisms and with different performance implications:
Factor
Foam Rolling
Static Stretching
Acute ROM effect
Large (d=0.76)
Large (similar)
Effect on strength performance
No negative effect
Temporary reduction if prolonged (>60 sec/muscle)
Best timing
Before training
After training or separate session
Combination effect
Rolling then stretching may produce greater ROM than either alone
Common Questions About Foam Rolling
How long should I foam roll each area?
Research suggests 30–90 seconds per muscle area for acute ROM effects.
For pre-training warm-up, 30–45 seconds is typically sufficient.
For post-training recovery or dedicated mobility sessions, 60–90 seconds allows more thorough tissue coverage.
Beyond 2 minutes per area, there is diminishing return — additional time does not proportionally increase the benefit.
Should foam rolling hurt?
Moderate discomfort (4–6 on a 10-point scale) is expected and appropriate — a feeling of “good pain” that eases during the rolling session is the typical experience.
Sharp, shooting, or electrical pain during foam rolling is not appropriate and may indicate contact with a nerve — repositioning or stopping is advisable.
Pain that is consistently 8–10/10 intensity typically means either the area has an underlying issue requiring medical assessment, or the pressure is excessive for that individual and should be reduced.
How often should I foam roll?
Daily foam rolling (5–15 minutes) is appropriate for most healthy adults and produces better long-term ROM outcomes than occasional sessions.
The research supporting lasting ROM improvements specifically notes that interventions longer than 4 weeks produce significantly better outcomes — implying that consistency over months matters more than session duration.
Even 5 minutes of daily rolling for key areas (thoracic spine, quads, hamstrings) may produce more lasting improvement than 30-minute sessions performed once or twice per week.
✅ Key Takeaways
Foam rolling reliably increases ROM acutely and produces lasting improvements with consistent practice over 4+ weeks
Pre-training foam rolling does not impair performance — unlike prolonged static stretching, making it a practical warm-up tool
The combination of foam rolling followed by static stretching may produce greater ROM than either alone
Moderate pressure (4–6/10 discomfort) is the target — extreme pain does not produce proportionally greater benefit
Foam rolling does not physically “break up adhesions” or produce lasting structural change from a single session
Building a Systematic Foam Rolling Practice: Protocols by Goal
For Athletes: Pre-Competition and In-Season Protocols
Athletes benefit from foam rolling’s performance-preservation properties — increasing ROM acutely without impairing strength or power output.
Pre-competition rolling (15–20 min before warmup):
Lower body athletes: Quads, hamstrings, glutes, calves — 45 sec per area
Upper body athletes: Thoracic spine, lats, posterior shoulder — 45 sec per area
Full body: Prioritize areas relevant to the sport’s primary movement demands
Post-competition recovery rolling (within 2 hours):
Muscles used most heavily during competition — 60–90 sec per area
Focus on areas of most notable fatigue or anticipated soreness
For General Fitness Trainees: The 4-Week Establishment Protocol
Week 1 (Daily, 8–10 min):
3 areas per session: thoracic spine + quadriceps + hamstrings | 60 sec each
Goal: establish the daily habit and learn proper pressure technique
Week 2 (Daily, 10–12 min):
Add glutes and calves | 60–90 sec each
Begin combining rolling with 30-second static stretches of rolled areas
Week 3–4 (Daily, 12–15 min):
Full protocol across all 7 target areas
Add IT band and lats on training-specific days
Assess ROM improvements compared to Week 1
For Desk Workers: The Daily Anti-Stiffness Protocol
Prolonged sitting creates predictable tightness patterns — thoracic spine kyphosis (increased rounding of the upper back), hip flexor shortening, and hamstring stiffness.
A targeted daily protocol addressing these specifically:
Morning or evening desk-worker routine (10 min):
✅ Thoracic extension over roller — 90 seconds (counteracts forward rounding)
✅ Quadriceps rolling — 60 seconds per leg (counteracts hip flexor shortening)
✅ Glute rolling — 60 seconds per side (activates inhibited glutes)
✅ Hip flexor stretch after rolling — 30 seconds per side
✅ Standing thoracic rotation — 10 reps each side (active mobility after rolling)
Foam Rolling for Older Adults and Special Populations
Foam rolling may be particularly beneficial for older adults — research shows that ROM tends to decline with age, and foam rolling provides a low-impact, accessible way to address this.
Modifications appropriate for older adults or those with limited mobility:
Using a softer foam roller or performing rolling on a mat rather than a hard floor — reduces pressure intensity
Seated modifications — some areas (calves, hamstrings) can be rolled from a chair using a massage ball or roller stick rather than floor-based positions
Shorter durations (30 seconds per area) initially — building tolerance before increasing duration
Individuals over 60, those with osteoporosis, or those with joint replacement should consult their healthcare provider or physiotherapist before beginning foam rolling to ensure appropriate areas and techniques are used safely.
Monitoring Progress in a Foam Rolling Program
Tracking foam rolling progress helps confirm the protocol is producing results and guides adjustments:
Sit-and-reach test: A standardized flexibility assessment measured monthly — improvements after 4–8 weeks of consistent rolling are typically measurable
Subjective tightness rating: A 1–10 rating of specific area tightness before each session — gradual decline over weeks indicates adaptation
Functional movement quality: Improvements in squat depth, lunge comfort, and overhead reach are practical indicators of mobility progress
The Long-Term Perspective
The most evidence-supported approach to foam rolling is treating it as a daily practice — not a pre-training ritual to occasionally remember and not an intensive weekly session.
The research on lasting ROM improvements specifically identifies interventions longer than 4 weeks as producing significantly better outcomes — implying that months of consistent daily practice, even at modest duration, produces more complete mobility improvement than any amount of intensive occasional rolling.
A qualified physiotherapist, sports massage therapist, or certified strength and conditioning specialist can assess specific mobility limitations and design a foam rolling protocol tailored to your individual anatomy, training demands, and mobility goals — particularly useful if chronic tightness in specific areas has not responded to general protocols after several weeks of consistent practice.
Integrating Foam Rolling With a Complete Mobility Program
Foam rolling is most effective as one component of a comprehensive mobility practice rather than a standalone solution.
A complete mobility program typically includes:
Foam rolling (self-myofascial release): Neural tone reduction, acute ROM preparation, soreness management
Static stretching: Sustained muscle lengthening — placed post-rolling or post-training
Dynamic mobility: Active movement through range — leg swings, hip circles, arm rotations — most appropriate immediately before training
Strength work at end range: Exercises like deep squats, hip 90/90 holds, and overhead reaches that build strength in the new range of motion achieved by stretching
The combination of these four components addresses mobility from multiple angles — neural, structural, and functional — producing more complete and durable flexibility improvements than any single modality alone.
Building each component into a consistent daily practice, even at 5 minutes each, compounds into meaningful flexibility improvements over months that single-modality approaches often fail to produce.
The rectus femoris is the quadriceps muscle that crosses two joints rather than one. While the vastus lateralis, vastus medialis, and vastus intermedius cross only the knee, the rectus femoris originates at the anterior inferior iliac spine of the pelvis and crosses both the hip and the knee. This two-joint architecture means the rectus femoris…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only. It does not replace professional medical advice. If you have existing shoulder pain, rotator cuff injury, or shoulder impingement, consult a qualified healthcare professional before starting any scapular training programme. Most shoulder problems in the gym do not start at the shoulder joint…
⚠️ Wrist Safety NoteWrist mobility exercises involving loaded extension or flexion place stress on the distal radius, carpal bones, and triangular fibrocartilage complex (TFCC). Individuals with active wrist tendinopathy, carpal tunnel syndrome, Kienbock’s disease, or a history of distal radius fracture within 12 months should obtain physiotherapy clearance before starting progressive wrist loading. Sharp or…
Tight hamstrings are the most commonly cited flexibility limitation in recreational athletes. They are also the most commonly treated incorrectly. The standard approach: stretch the hamstrings for 30 seconds, three times, after training. Sometimes before training. Consistently for a few weeks, then irregularly, then not at all, because nothing seems to change. The hamstrings feel…
Calf tightness is one of the most widespread and most underaddressed mobility restrictions in recreational athletes. Most trainees know their calves are tight. Few understand specifically what that tightness limits or how to resolve it systematically. Restricted calf flexibility means restricted ankle dorsiflexion: the ability to bring the foot toward the shin during loaded movement….
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. The Fitness Quality Nobody Trains Until It Fails Them Balance is…