You foam roll the IT band. It hurts. It feels slightly better for 20 minutes. The next run, it hurts again in the same place at the same point in the stride. You foam roll again. The cycle continues for months.
This pattern is the defining experience of IT band syndrome. The treatment that everyone recommends produces temporary relief and no lasting change. The reason is that most IT band treatment addresses the wrong structure through the wrong mechanism.
This guide covers what the research actually shows about why IT band syndrome develops, why foam rolling the IT band itself produces limited benefit, what actually causes the syndrome, and the systematic approach that produces lasting resolution rather than temporary symptom management.
What IT Band Syndrome Actually Is and Why the Friction Theory Is Wrong
The Anatomy of the IT Band
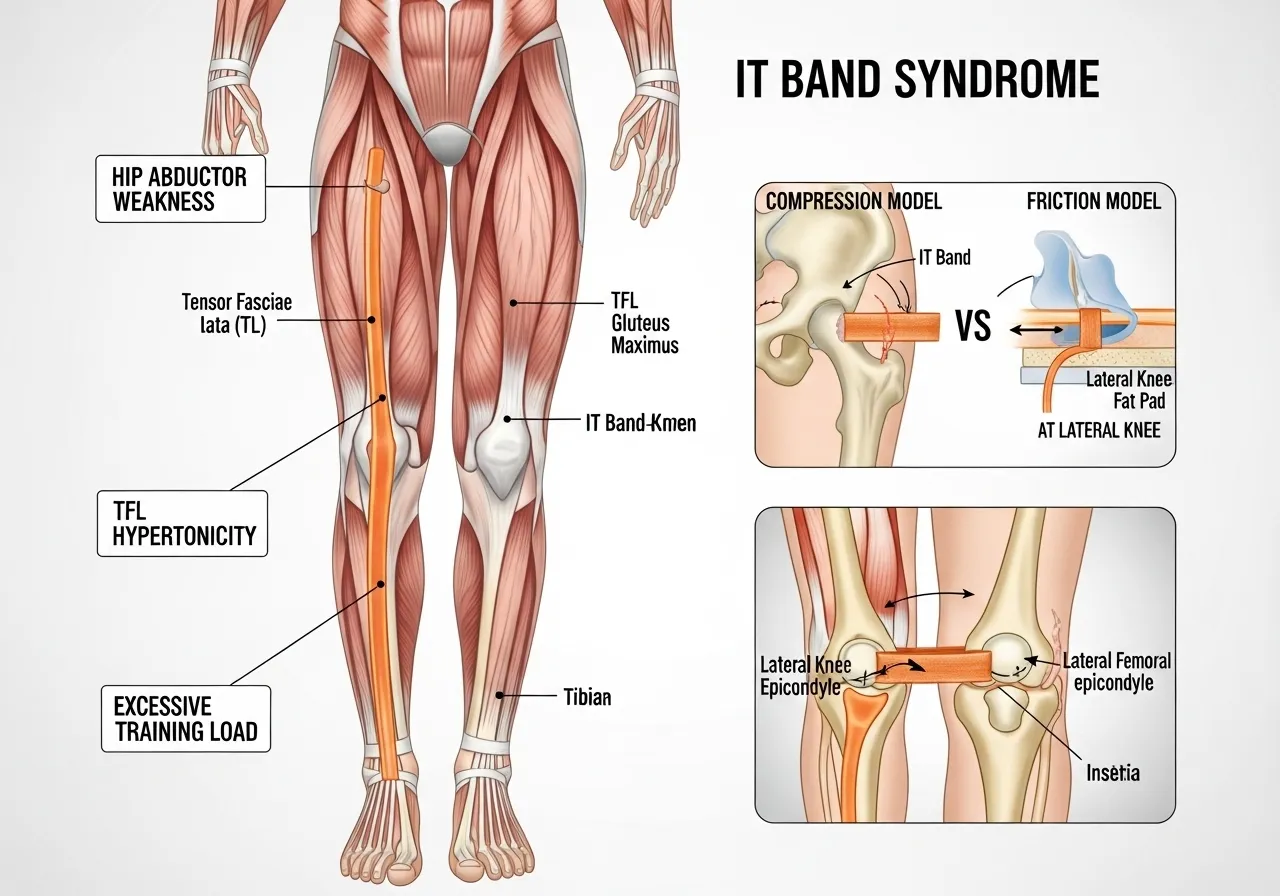
The iliotibial band is a thick strip of dense connective tissue running from the iliac crest of the pelvis, down the lateral thigh, and inserting at Gerdy’s tubercle on the lateral tibial condyle. It is not a muscle. It has no contractile tissue. It cannot be stretched in the conventional sense because connective tissue of this density does not meaningfully elongate under the loads applied during stretching or foam rolling.
The IT band is continuous with the tensor fascia latae at the hip and receives contributions from the gluteus maximus. It functions as a lateral stabiliser of the knee and hip during the stance phase of running and cycling, transmitting forces rather than generating them.
Compression, Not Friction: The Revised Understanding
For decades, IT band syndrome was explained as friction between the IT band and the lateral femoral condyle during repetitive knee flexion and extension. Treatment logically focused on stretching and rolling to reduce this friction.
More recent biomechanical research has revised this model. The IT band does not move anteriorly and posteriorly over the condyle in the way the friction model requires. It compresses against a fat pad in the lateral knee during the impingement zone of 20 to 30 degrees of knee flexion. The syndrome is caused by compressive force on the fat pad beneath the IT band, not friction on the IT band itself.
This distinction is clinically significant. You cannot foam roll compressive force out of a fat pad. You cannot stretch away the hip abductor weakness that creates the excessive lateral knee stress. The structural causes require structural solutions.
What Actually Causes IT Band Syndrome
A review of the iliotibial band syndrome etiology and risk factors found that ITBS is one of the most common overuse syndromes causing knee pain, especially prevalent in runners and also common in cyclists, rowers, and field athletes, with the literature on etiology and risk factors conflicting and inconclusive but consistently identifying training load errors, hip abductor weakness, and running biomechanics as primary contributing factors.
The mechanical causes are well established even if the tissue mechanism is debated:
Hip abductor weakness: Insufficient gluteus medius strength allows the femur to adduct excessively during stance, increasing compressive load at the lateral knee
Training load errors: Too much volume too quickly, particularly in runners who increase weekly mileage faster than connective tissue can adapt
Running surface and footwear: Camber running, repetitive downhill running, and inadequate footwear cushioning all increase lateral knee compressive forces
Tensor fascia latae tightness: TFL hypertonicity pulls the IT band into greater tension, increasing compression at the knee
📌 Key Finding
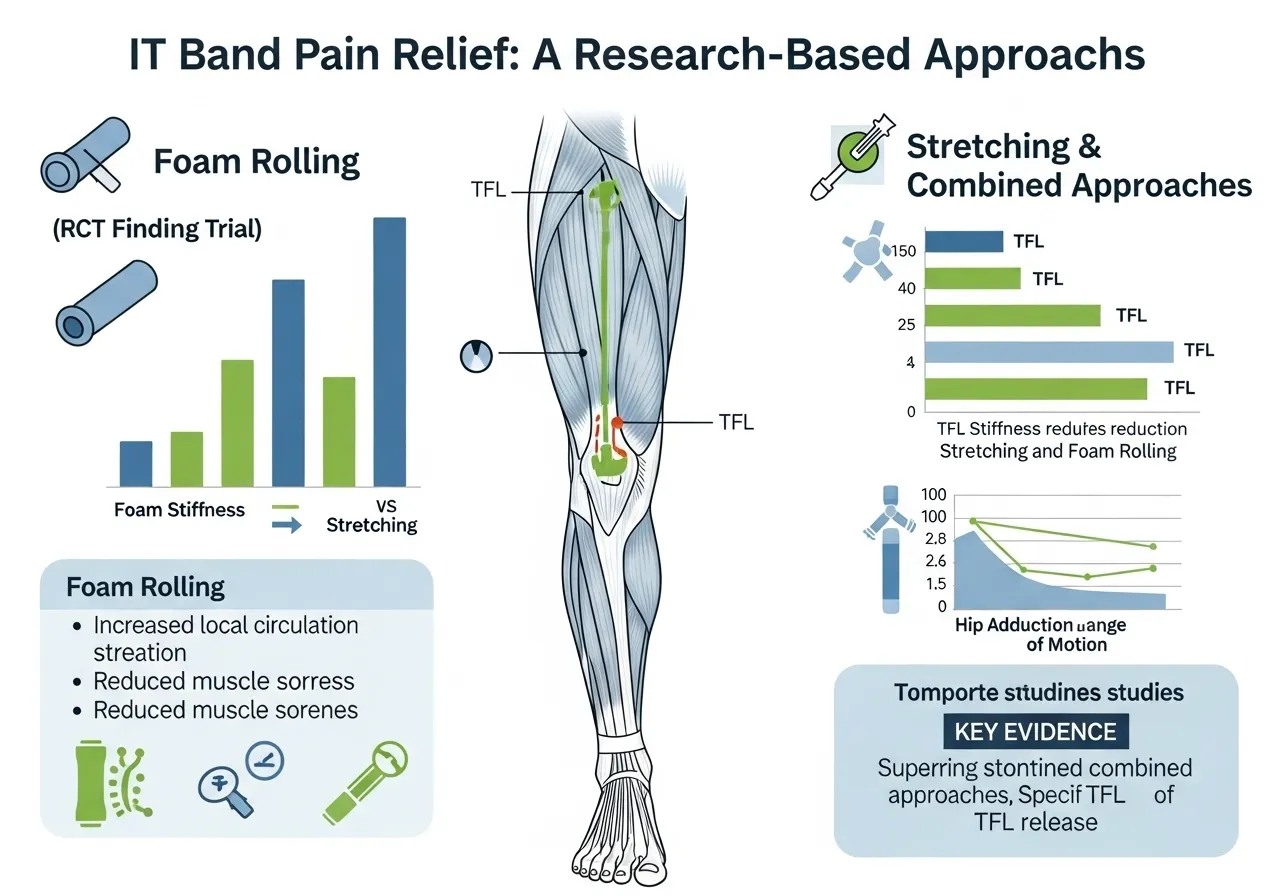
Foam rolling reduces IT band stiffness acutely. Stretching improves hip adduction range. Neither addresses the hip abductor weakness or training load errors that cause the syndrome. Both are symptom management tools, not resolution strategies, when used in isolation.
The Narrative Review Evidence: What Actually Works
📌 Key Finding
There is no consensus on standard ITBS care. Stretching and foam rolling provide symptomatic relief but do not address biomechanical causes. A complete resolution strategy requires addressing hip abductor weakness and training load management alongside soft tissue work.
The Role of the IT Band Foam Rolling in a Complete Protocol
Foam rolling the IT band is not useless. It reduces acute stiffness, decreases perceived tightness before and after activity, and provides short-term symptomatic relief that allows training to continue at reduced intensity during resolution.
The error is treating foam rolling as the treatment rather than one component of a multi-targeted approach. Foam rolling the IT band daily while ignoring gluteus medius weakness and continuing the training load that caused the syndrome is why ITBS persists for months in otherwise diligent trainees.
Self-Assessment: How to Identify the Specific Causes in Your Case
The Ober Test: Assessing IT Band and TFL Tightness
The Ober test assesses IT band and TFL tightness. Lie on your side with the unaffected leg down. Bring the top leg into hip extension and abduction (raised out to the side). If the top leg cannot lower toward the table under gravity while the hip remains in extension, the IT band and TFL are significantly restricted.
A modification: if the hip must flex forward to allow the leg to lower, this indicates TFL tightness specifically (the TFL is a hip flexor as well as an abductor). If the leg can lower when the hip flexes but not in true extension, TFL flexibility is the primary limiting factor over IT band stiffness.
Hip Abductor Strength Test
Stand on one leg and observe hip position. In a well-functioning hip abductor system, the pelvis remains level during single-leg stance. If the opposite hip drops (Trendelenburg sign), the standing leg’s gluteus medius is insufficient to maintain pelvic level.
A more sensitive test: perform 10 single-leg squats on each side and observe knee tracking. If the knee of the squatting leg collapses medially toward the midline, hip abductor weakness is the primary biomechanical driver of lateral knee stress. This is the most reliable predictor of ITBS in runners and should be the primary focus of any resolution programme. Strengthening the gluteus medius and hip external rotators is covered systematically in the glute activation guide.
Training Load Assessment
ITBS almost universally involves a training load error. The relevant questions are:
Did weekly running or cycling volume increase by more than 10% in the three to four weeks before symptoms appeared?
Was there a sudden introduction of hill or stair work?
Was there a change in footwear or running surface around the time of onset?
Were back-to-back training days added without recovery days between?
Identifying the specific load error is essential because returning to that same load pattern after symptom resolution will reproduce ITBS. The load that caused the syndrome must be identified and managed, not simply rested through until symptoms resolve spontaneously.
6 Exercises That Actually Resolve IT Band Syndrome
⚠️ ITBS and Pain Management Note These exercises are for individuals with ITBS who have a confirmed diagnosis or whose lateral knee pain matches the classic ITBS presentation: pain at the lateral knee at 20 to 30 degrees of flexion during running or cycling, worsening with activity continuation. Sharp radiating pain, locking, or swelling may indicate a structural knee pathology requiring medical assessment before exercise. Acute ITBS flare-ups require a period of reduced load before rehabilitation exercises begin.
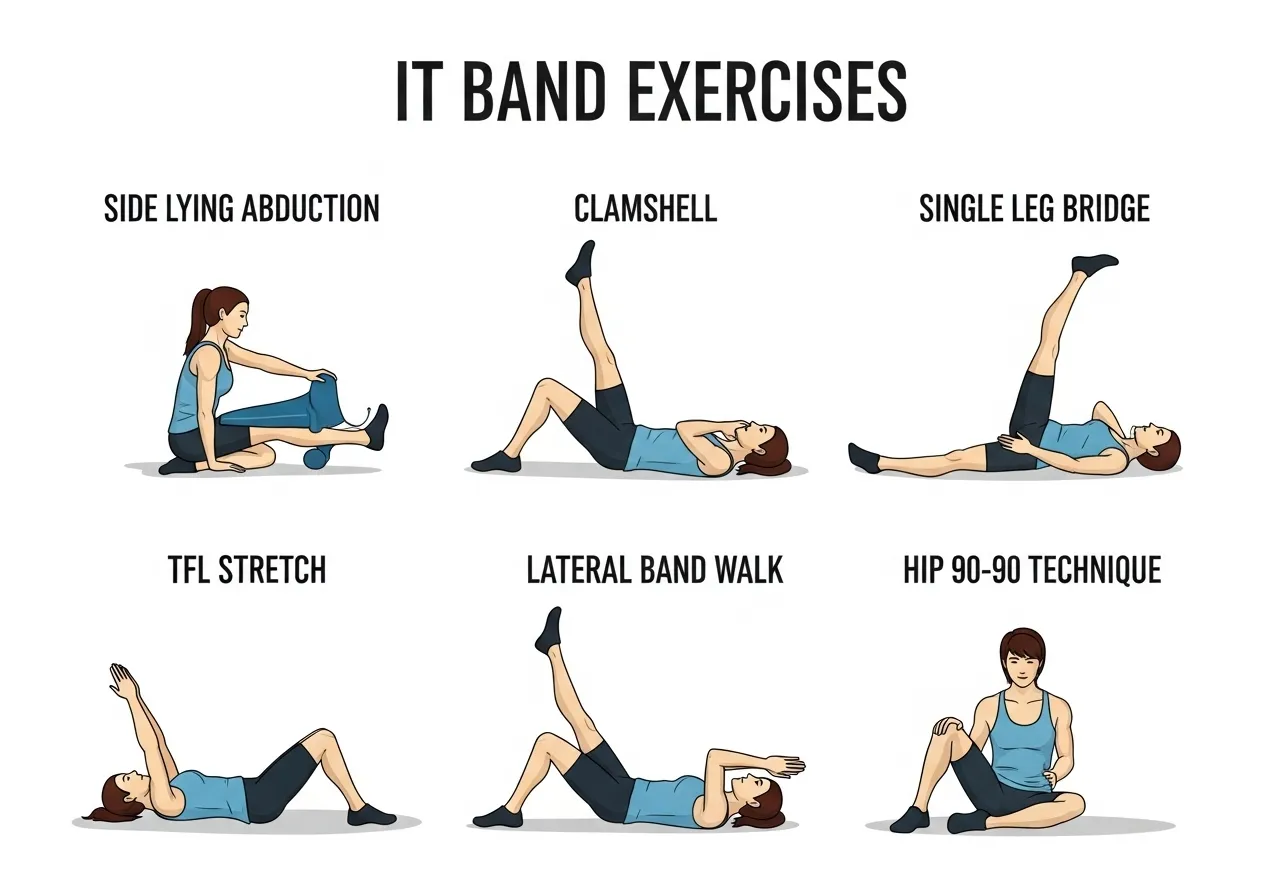
🔵 1. Side-Lying Hip Abduction
Target: Gluteus medius, hip abductors, pelvic stability
How: Lie on your side with the bottom leg slightly bent. Keeping the top leg straight and the foot parallel to the floor (not rotated up), raise the top leg to approximately 30 degrees. Hold 2 seconds at the top. Lower under control. Progress by adding a resistance band above the knees.
Key point: Do not rotate the hip to allow a higher lift. The external rotation compensation means the TFL is doing the work, not the gluteus medius. The foot should remain parallel throughout.
🔵 2. Clamshell with Band
Target: Gluteus medius, hip external rotators
How: Lie on your side with hips and knees bent at 45 degrees, resistance band above the knees. Rotate the top knee upward against band resistance while keeping the feet together. Hold 1 to 2 seconds at the top. Return under control.
Key point: The pelvis must not roll backward during the movement. A pelvis rock signals that the hip external rotators have reached their end range and compensation is occurring. Reduce range of motion before adding band resistance.
🔵 3. Single-Leg Bridge
Target: Gluteus maximus and medius, hip stability under pelvic asymmetry
How: Lie on your back with knees bent. Extend one leg straight. Drive through the grounded heel to lift the hips. At the top, both hips should be level. If the unsupported hip drops, the working side gluteus medius is insufficient. Hold 2 seconds at the top.
Key point: Hip drop at the top is the diagnostic finding for hip abductor insufficiency that drives ITBS. Do not correct the drop by tilting the pelvis; reduce range and maintain level hips throughout.
🔵 4. TFL Stretch (Standing)
Target: Tensor fascia latae, IT band complex, lateral hip
How: Stand beside a wall with the affected side toward the wall. Cross the affected leg behind the unaffected leg. Lean your hip toward the wall while keeping both feet flat on the floor. The stretch should be felt on the lateral hip and upper thigh of the rear leg. Hold 30 to 60 seconds.
Key point: The key is the hip adduction in the crossed position, not spinal side-bending. If you achieve the stretch by bending sideways at the waist, the TFL is not in the correct position to be lengthened. Focus on pushing the hip toward the wall.
🔵 5. Lateral Band Walk
Target: Gluteus medius, dynamic hip abduction stability
How: Place a resistance band above the knees. Stand with feet hip-width and slight knee bend. Step sideways maintaining band tension throughout, keeping the torso upright and not leaning toward the stepping foot. Perform 12 to 15 steps each direction.
Key point: The step must maintain band tension through the entire movement. Trunk lean toward the stepping leg is the compensation for insufficient gluteus medius. Keep shoulders level and drive the step from the hip abductors, not from body weight shift.
🔵 6. Hip 90-90 Stretch with Lateral Bias
Target: Hip external rotators, posterior lateral hip capsule, piriformis
How: Sit with one leg bent at 90 degrees in front and the other bent at 90 degrees to the side. Lean forward over the front shin while keeping the torso upright. For the lateral bias, add a gentle lean toward the front leg to increase the external rotation stretch. Hold 45 to 60 seconds each side.
Key point: The lateral hip tightness that accompanies ITBS often extends into the deep external rotators and piriformis. This stretch addresses the posterior lateral hip structures that direct TFL stretches miss.
The Real Reason IT Band Syndrome Keeps Coming Back After Treatment
The Return-to-Running Error
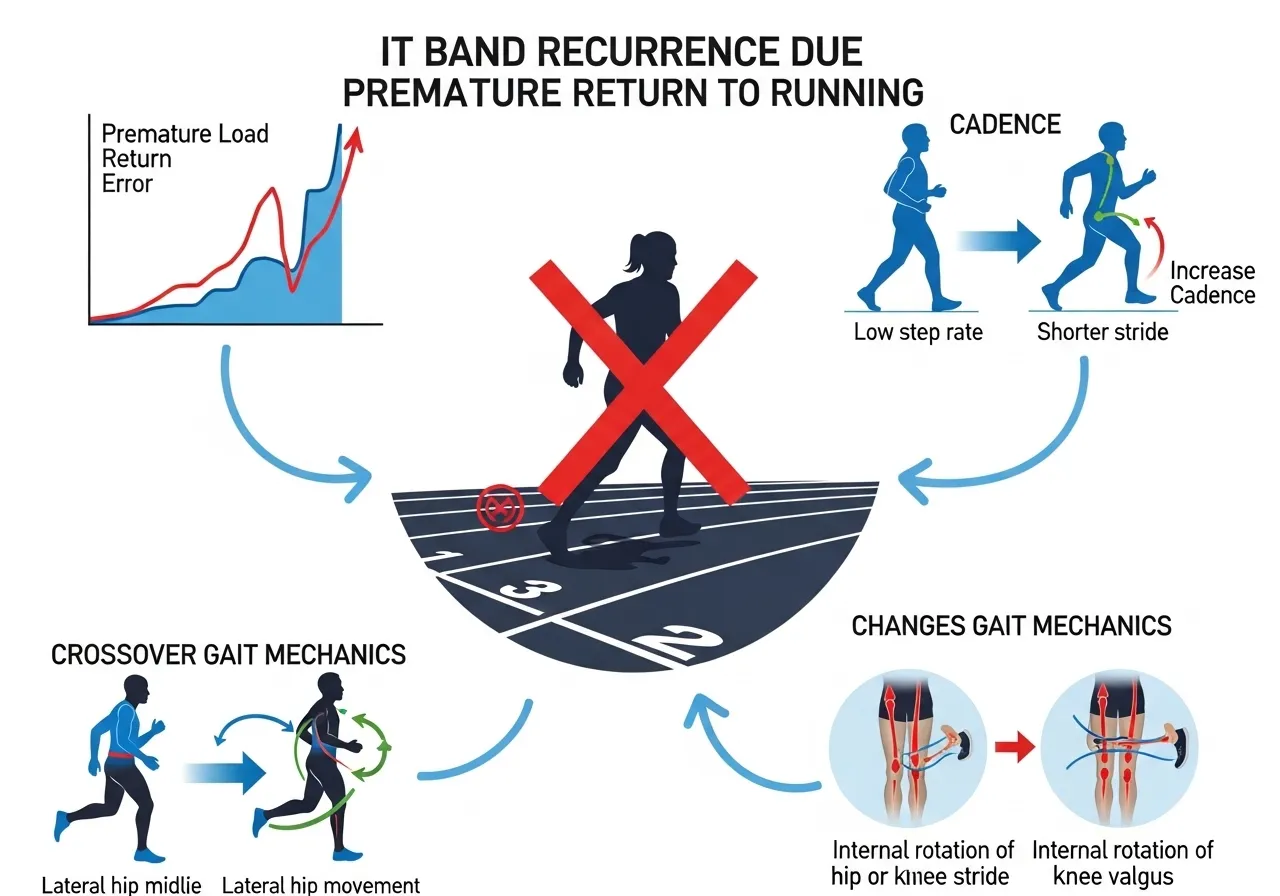
The most common reason ITBS recurs after apparent resolution is premature return to the training volume that caused it. Symptoms resolve with rest and soft tissue work within two to four weeks. The athlete returns to running at the same load that produced the syndrome. Symptoms return within two to three weeks.
Symptom resolution is not structural resolution. The hip abductor weakness that allowed excessive femoral adduction during stance is still present when pain resolves. The TFL hypertonicity that increased IT band tension is still present when pain resolves. The training load error is still the default training pattern.
Returning to running before completing six to eight weeks of progressive hip strengthening and before identifying and managing the specific load error that caused the syndrome guarantees recurrence for most trainees.
The Training Load Re-Entry Protocol
When returning to running after ITBS, the appropriate re-entry protocol is significantly more conservative than most trainees attempt:
Week 1 to 2: Return at 30 to 40% of the volume at which symptoms appeared. No hills. No back-to-back running days.
Week 3 to 4: Increase to 50 to 60% of previous volume only if completely symptom-free. Continue hip strengthening as a warmup before every run.
Week 5 to 8: Progress toward previous volume by no more than 10% per week.
Any return of lateral knee pain during this protocol requires an immediate step back to the previous week’s volume. Pain during the re-entry phase is a signal that hip strengthening has not progressed sufficiently to support the running load, not simply that more rest is needed.
The Biomechanics That Must Change
Runners with ITBS who return to running without addressing their running mechanics will recur at the same volume that originally caused ITBS. The specific mechanical changes associated with reduced ITBS recurrence are:
Reduced ipsilateral trunk lean during stance
Increased cadence (steps per minute), which reduces peak knee adduction angle
Reduced crossover gait (landing with the foot crossing the midline)
Increasing running cadence by 5 to 10% from the individual’s natural cadence is one of the most evidence-supported running mechanics changes for ITBS prevention and is accessible without formal gait retraining. Ankle mobility directly affects running mechanics. Restricted dorsiflexion forces compensatory pronation and tibial internal rotation that increases lateral knee stress. The ankle dorsiflexion work relevant to running mechanics is covered in the ankle mobility guide.
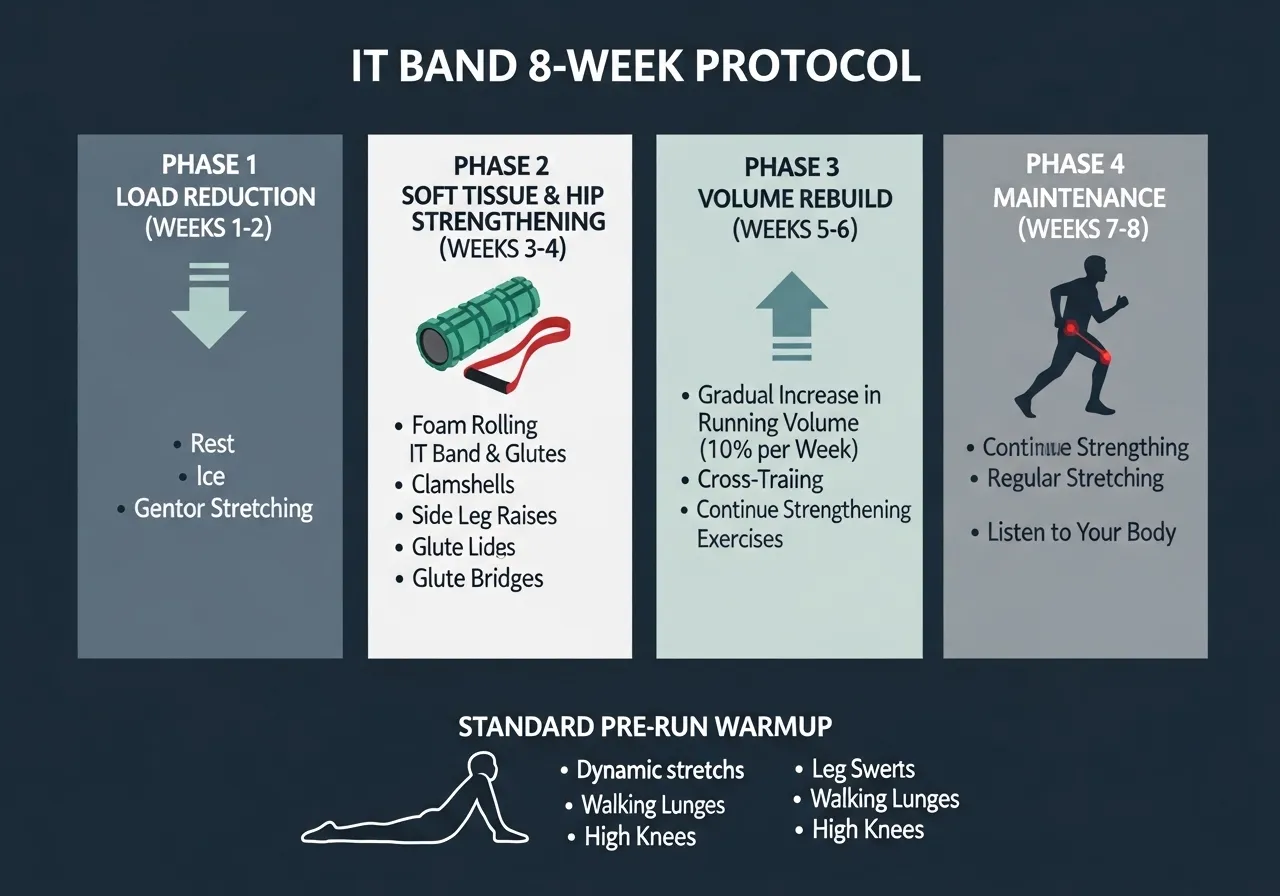
8-Week IT Band Syndrome Resolution Protocol
📅 Phase 1: Weeks 1 to 2: Load Reduction and Soft Tissue Work
Reduce running or cycling volume by 50 to 70%
IT band foam rolling: 2 minutes per side, twice daily
TFL standing stretch: 3 sets of 45 seconds per side, twice daily
Hip 90-90 stretch: 2 sets of 45 seconds per side, daily
No exercise that produces lateral knee pain above 2 out of 10
Focus: Reduce compressive load at the lateral knee while beginning soft tissue normalisation. Do not push through pain in this phase.
📅 Phase 2: Weeks 3 to 4: Hip Strengthening Introduction
Continue Phase 1 soft tissue work once daily
Side-lying hip abduction: 3 sets of 15 per side
Clamshell with light band: 3 sets of 12 per side
Single-leg bridge: 3 sets of 10 per side
Maintain reduced running volume with no increase yet
Focus: Begin developing the hip abductor capacity that prevents recurrence. Initial hip strengthening soreness is expected and does not indicate worsening of the ITBS.
📅 Phase 3: Weeks 5 to 6: Load and Volume Rebuild
Progress hip exercises: add resistance band to abduction and clamshell
Add lateral band walk: 3 sets of 12 steps each direction
Begin conservative return to running: 30 to 40% of original volume
Perform hip strengthening warmup before every run session
Continue TFL and 90-90 stretching pre-run
Focus: Combine hip strengthening with conservative running re-entry. Any return of lateral knee pain during runs requires immediate load reduction.
📅 Phase 4: Weeks 7 to 8: Progressive Return and Maintenance Standard
Progress running volume by no more than 10% per week if symptom-free
Maintain hip strengthening as a permanent pre-run warmup (10 minutes)
Establish the hip abduction and clamshell exercises as indefinite training practice
Introduce single-leg squats to test hip abductor capacity under functional load
Target: symptom-free running at 70 to 80% of original volume by end of Week 8
Focus: Establish maintenance practices that prevent recurrence. The hip strengthening warmup is not temporary rehabilitation; it becomes the permanent pre-run standard.
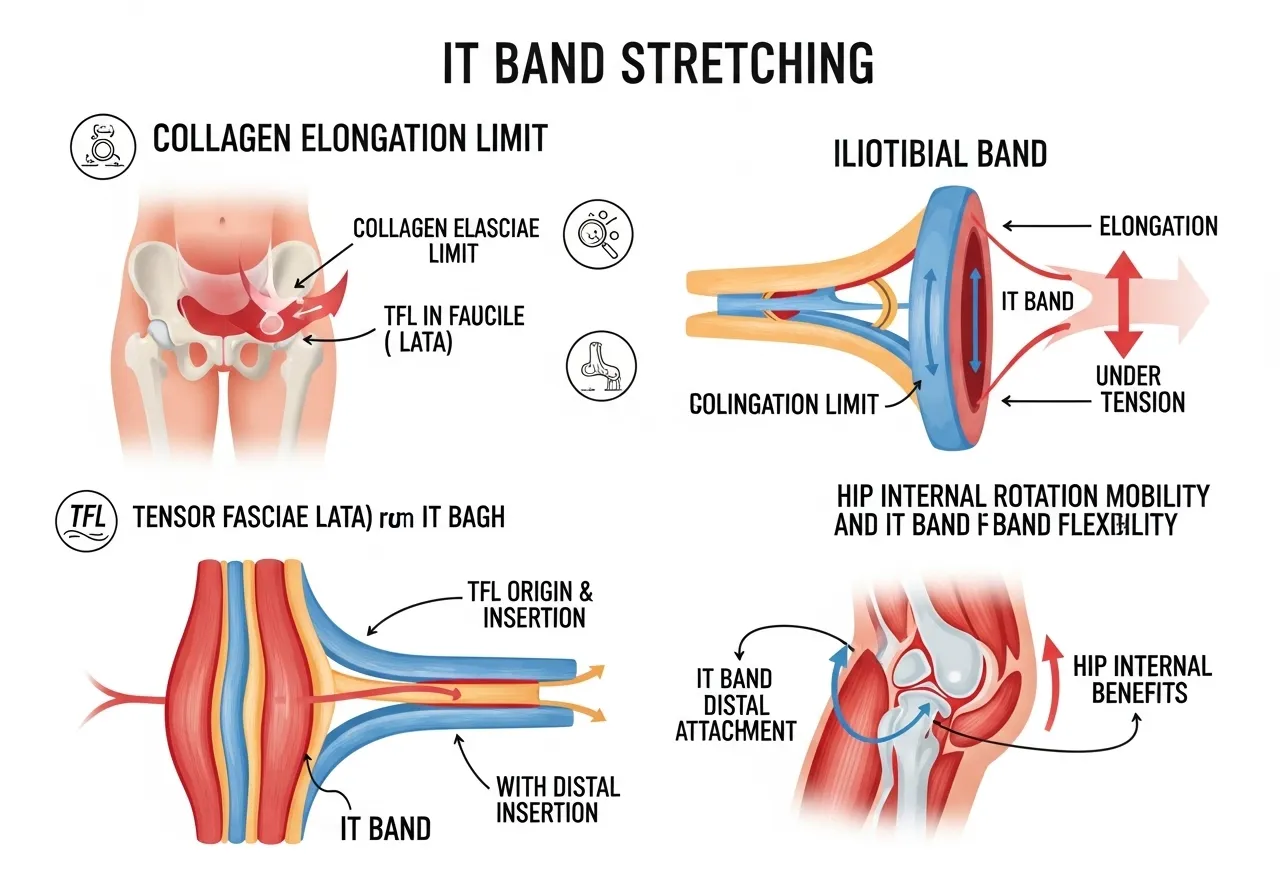
Is Stretching the IT Band Directly Even Possible?
The Structural Reality
The iliotibial band is composed of dense fibrous connective tissue, primarily type I collagen, with a tensile strength that exceeds most human muscular force production capacity. The mechanical forces applied during stretching and foam rolling are insufficient to produce meaningful elongation of the IT band itself.
This does not mean IT band stretching is useless. Standard “IT band stretches” predominantly stretch the TFL and the tensor-band junction at the hip, not the IT band directly. This is why the Ober test responds better to hip flexion manipulation than to direct IT band stretching: what changes is TFL length and hip capsule mobility, not IT band length.
The distinction matters for treatment selection. If the primary restriction is TFL tightness, standing TFL stretches and hip adduction mobility work directly address the cause. If the primary restriction is hip capsule tightness limiting adduction range, joint mobilisation and hip 90-90 work are more appropriate. If the primary problem is hip abductor weakness allowing excessive femoral adduction, no amount of stretching addresses the cause.
The Hip Mobility Connection
Lateral hip tightness is often a secondary symptom of restricted hip internal rotation range. When the hip lacks internal rotation range, the femur compensates by adducting and internally rotating through alternative movement pathways, increasing lateral knee stress during the stance phase of running. Addressing hip internal rotation mobility reduces the compensatory demands that manifest as lateral knee pain. The hip mobility work that addresses the full rotation range, including internal rotation deficits, is covered in the hip mobility guide.
Frequently Asked Questions About IT Band Syndrome
How long does IT band syndrome take to resolve?
With a systematic approach addressing hip strengthening, load management, and soft tissue work simultaneously, most individuals achieve symptom-free running within six to eight weeks. Trainees who use only soft tissue work without addressing hip weakness and load errors typically experience recurring symptoms over months to years.
The fastest recovery occurs in individuals who identify and correct the specific training load error early, begin hip strengthening before returning to full training volume, and maintain hip strengthening as a permanent running warmup after resolution. Delayed treatment or premature return to full training volume are the primary reasons recovery extends beyond eight weeks.
Should I stop running completely with IT band syndrome?
Complete rest is rarely necessary and counterproductive for most ITBS presentations. The more effective approach is significant load reduction, typically 50 to 70% of the volume at which symptoms appeared, while beginning hip strengthening and soft tissue work simultaneously.
Complete rest allows symptoms to resolve temporarily but does nothing to address the hip weakness and mechanics that caused the syndrome. Trainees who rest completely and then return to full training at the same load will recur. Modified training at reduced volume while building hip capacity is both more practical and more effective than complete rest.
Why does my IT band hurt going down stairs and not up?
Stair descent involves controlled knee flexion through the 20 to 30 degree range where ITBS compressive force is highest. The eccentric quadriceps contraction required to control descent increases ground reaction forces and prolongs time in the impingement zone. Stair ascent involves quicker movement through this range with less eccentric loading, producing less compression at the lateral fat pad.
This pattern, pain on descent but not ascent, is one of the most reliable indicators of ITBS rather than other lateral knee pathologies. It confirms that compressive force at 20 to 30 degrees of knee flexion is the primary pain mechanism.
Can I continue cycling with IT band syndrome?
Cycling produces ITBS through the same compressive mechanism as running. The repetitive knee flexion-extension through the impingement zone during pedalling aggravates the lateral fat pad with each stroke. Saddle height is a particularly important cycling variable: a saddle set too low increases the peak knee flexion angle and time spent in the compressive zone.
Raising saddle height by 5 to 10 mm reduces peak knee flexion angle and is one of the most accessible interventions for cyclists with ITBS. This alone resolves ITBS for many cyclists whose saddle height was the primary contributing factor. If symptoms persist after saddle height optimisation, the hip strengthening and load reduction protocol applies identically to cycling as to running.
Key Takeaways
IT band syndrome is caused by compressive force on the lateral knee fat pad, not friction. Foam rolling reduces stiffness acutely but does not address the compression mechanism.
Foam rolling targets the IT band directly; stretching primarily targets the TFL. Both provide symptomatic relief but neither resolves hip abductor weakness or training load errors.
Hip abductor weakness allowing excessive femoral adduction during stance is the primary biomechanical driver of ITBS. Gluteus medius strengthening is the most important structural intervention.
Returning to running before completing six to eight weeks of progressive hip strengthening guarantees recurrence for most trainees.
Increasing running cadence by 5 to 10% reduces peak knee adduction angle and is one of the most evidence-supported mechanical interventions for ITBS prevention.
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only. It does not replace professional medical advice. If you have existing shoulder pain, rotator cuff injury, or shoulder impingement, consult a qualified healthcare professional before starting any scapular training programme. Most shoulder problems in the gym do not start at the shoulder joint…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only and does not replace professional medical advice. If you have any pre-existing joint, spinal, or cardiovascular conditions, please consult a qualified healthcare professional before beginning a yoga practice. Yoga occupies a unique position among fitness modalities — simultaneously developing flexibility, balance training guide,…
Sciatica is one of the most common causes of persistent lower body pain in active adults, and radiating arm pain from cervical nerve compression is its upper body equivalent. Both conditions share a mechanism: the peripheral nerve is irritated, compressed, or has lost its normal ability to glide freely through the surrounding tissues. Movement that…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program. ⚠️ Medical Disclaimer: This article is for general informational purposes only. If you are experiencing joint pain or any health…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only and does not replace professional medical advice. If you have any spinal, pelvic, or chronic pain conditions, please consult a qualified healthcare professional before beginning a Pilates program. Pilates occupies a unique position in the fitness landscape — simultaneously a rehabilitation tool used…
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only.It does not replace professional medical or fitness advice.If you have any pre-existing injury, chronic pain, or health condition — please consult a qualified healthcare professional before starting or modifying any stretching or flexibility program. Stretching is one of the most universally…