⚠️ Breathing and Cardiovascular Safety Note Breathing exercises involving breath-holding (Valsalva manoeuvre variants) and hyperventilation drills significantly alter blood pressure and carbon dioxide levels. Individuals with uncontrolled hypertension, a history of syncope (fainting), cardiovascular disease, or epilepsy should avoid high-intensity breath-holding exercises and obtain medical clearance before starting structured diaphragmatic breathing training. Dizziness or tingling during breathing exercises indicates hyperventilation — return to normal breathing immediately and do not attempt the drill again without guidance.
You breathe approximately 20,000 times per day.
Most of those breaths are inefficient. The chest rises instead of the belly expanding. The diaphragm barely contracts. The accessory muscles of the neck and shoulders do the work instead of the primary breathing muscle doing its job.
Dysfunctional breathing patterns do not just reduce oxygen efficiency — they directly compromise core stability, elevate resting muscle tension, and limit athletic performance in ways that no amount of stretching or strengthening addresses. This guide identifies whether you have a dysfunctional breathing pattern, explains the mechanisms through which breathing affects strength and stability, and provides the exercises and programme that produce genuine change.
Self-Diagnosis: Is Your Breathing Pattern Limiting Your Training?
The Breathing Assessment
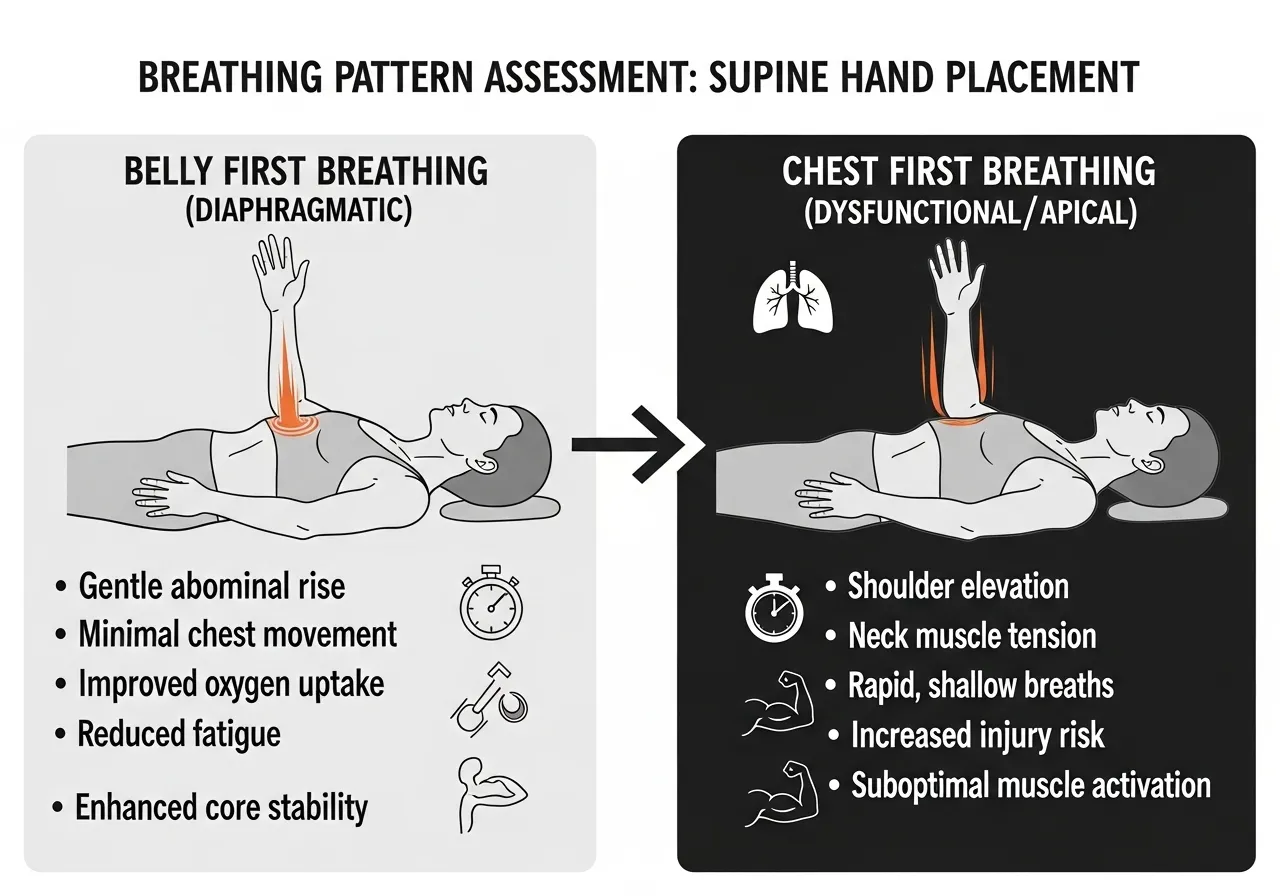
Lie on your back with one hand on your chest and one on your belly. Breathe normally for 30 seconds and observe which hand moves first and most on each inhale.
Normal diaphragmatic breathing: the belly hand rises first and largest on each inhale. The chest hand remains mostly still or rises slightly after the belly.
Dysfunctional chest breathing: the chest hand rises first and largest. The belly either stays still or moves minimally. This pattern indicates the diaphragm is underactivated and the accessory breathing muscles (scalenes, sternocleidomastoid, pectoralis minor) are performing most of the respiratory work.
Three Signs Your Breathing Pattern Affects Training Performance
Cannot brace effectively under heavy load: The intra-abdominal pressure spike that protects the spine during heavy lifting requires full diaphragmatic contraction. Chest breathers cannot generate adequate intra-abdominal pressure — leading to lower back vulnerability under load despite adequate abdominal muscle strength.
Chronic neck and upper trap tension: Accessory breathing muscles attach to the cervical spine and first ribs. Overusing them for every breath creates chronic tension in the upper trapezius, scalenes, and suboccipitals — the muscles most associated with tension headaches and neck pain in desk workers.
Rapid breathing fatigue during moderate exercise: Dysfunctional breathers reach their ventilatory threshold earlier during exercise because the respiratory system is operating less efficiently. The breathing muscles fatigue and compete with the working muscles for blood flow at lower exercise intensities than they should.
The Sitting Posture Connection
Extended sitting compresses the abdomen and forces the diaphragm upward into a shortened position — mechanically preventing full diaphragmatic excursion. Over months and years of prolonged sitting, the diaphragm adapts to this shortened position and loses its capacity for full range contraction even during standing and exercise.
This is why breathing dysfunction is so prevalent in sedentary populations and office workers — not because of any specific injury or pathology, but because of the postural environment that reduces diaphragmatic range of motion throughout most of the waking day.
The Breathing-Posture-Pain Triangle
Dysfunctional breathing, poor posture, and chronic pain form a reinforcing triangle — each perpetuating the others.
Forward head posture and rounded shoulders restrict thoracic expansion, reducing diaphragmatic room to descend. Restricted diaphragm causes accessory breathing muscle overuse. Accessory muscle overuse creates chronic tension in the neck and upper shoulder. Neck and shoulder tension reinforces the forward head posture that started the cycle.
Addressing any one component without the others produces partial improvement. Posture correction alone cannot restore diaphragmatic function if the breathing pattern remains dysfunctional. Breathing retraining alone cannot fully resolve neck tension if the postural mechanics that restrict thoracic expansion are not also addressed. The most effective approach treats breathing pattern, thoracic mobility, and postural alignment as a single interconnected system. See also: thoracic mobility guide — the most direct intervention for the restricted rib cage expansion that limits full diaphragmatic range.
What the Research Shows: Diaphragm Training, Core Stability, and Lower Back Pain
📌 Key Finding
The diaphragm is the primary core stability muscle — it creates intra-abdominal pressure before any limb movement. Dysfunctional breathing means the core cannot fully stabilise the spine, regardless of how strong the abdominals are.
📌 Key Finding
Chronic lower back pain is associated with reduced diaphragm thickness and movement. Breathing training directly improves back pain outcomes — not as a stretch or strengthening exercise, but by restoring the core stability mechanism the diaphragm provides.
📌 Key Finding
Breathing muscle training improves VO2max and endurance performance independently of other training. The respiratory system is a trainable performance limiter — not a fixed physiological constant.
The Pelvic Floor Connection: Breathing as a Complete System
The diaphragm does not work alone. It functions as the top boundary of a pressurised canister — with the pelvic floor as the bottom, the transversus abdominis as the sides, and the multifidus as the back wall. All four structures contract simultaneously during a proper diaphragmatic inhale and brace.
This means pelvic floor dysfunction and diaphragm dysfunction are often co-occurring — a leaky pelvic floor during exercise frequently indicates the entire pressure canister is not coordinating correctly, not just a local pelvic floor weakness. Treating breathing mechanics as an isolated component misses this systemic relationship. Trainers and physiotherapists who address all four structures together — diaphragm, transversus abdominis, pelvic floor, and multifidus — produce more complete and durable improvements in core stability than those addressing any single component in isolation.
For gym trainees without pelvic floor symptoms, this means breathing pattern improvement produces spillover benefits to the entire core stability mechanism — including the deep abdominals and spinal stabilisers that heavy barbell training depends on.
Can You Really Improve Athletic Performance Just by Breathing Differently?
The Sceptic’s Objection
The claim that breathing technique affects strength performance sounds like wellness marketing rather than exercise science. Most serious trainees associate breathing advice with yoga classes and mindfulness apps — not with squatting heavy or running faster.
The scepticism is understandable. But the mechanisms are concrete: intra-abdominal pressure, respiratory muscle fatigue, and autonomic nervous system state each have measurable effects on force production, endurance capacity, and recovery rate.
The Valsalva Manoeuvre: Already Used by Every Serious Lifter
Every experienced powerlifter and Olympic weightlifter already applies breathing science deliberately — they just call it the Valsalva. The Valsalva manoeuvre (inhale, close the glottis, brace the core) produces maximum intra-abdominal pressure that protects the spine under maximal loads.
The Valsalva requires a full diaphragmatic inhale to work correctly. A chest breather who attempts a Valsalva cannot generate adequate intra-abdominal pressure because the diaphragm never descends far enough to contribute its share of the pressure mechanism. Improving diaphragmatic breathing directly improves the Valsalva — and therefore directly improves spinal stability under maximum loads.
Respiratory Muscle Fatigue as a Limiting Factor
During hard exercise, the diaphragm and intercostal muscles compete with the legs, arms, and cardiovascular system for blood flow. When the respiratory muscles fatigue — which occurs progressively during sustained high-intensity effort — the body actually reduces blood flow to the working muscles to prioritise the respiratory system.
This “metaboreflex” is a real and measurable phenomenon. Stronger, more efficient respiratory muscles reduce the oxygen cost of breathing at any given intensity — delaying the metaboreflex and allowing more blood to reach the working muscles longer. The meta-analysis showing improved endurance performance from breathing training demonstrates this effect directly. See also: VO2max guide for how respiratory efficiency integrates into the full picture of aerobic capacity development.
The Autonomic Nervous System Effect
Slow, diaphragmatic breathing activates the parasympathetic nervous system — reducing cortisol, lowering heart rate, and improving recovery rate between hard efforts. Fast, shallow chest breathing maintains sympathetic activation — keeping the body in a stress state that limits recovery between sets, between sessions, and over training blocks.
Trainees who implement deliberate slow breathing between sets and during warm-up periods show improved performance consistency within sessions compared to trainees who breathe shallowly throughout — a finding that requires no expensive equipment to implement.
The CO2 Tolerance Factor: Why Breathing More Is Not Always Better
Chronic over-breathing — taking more breaths per minute or larger breaths than physiological demand requires — progressively reduces CO2 tolerance. Carbon dioxide, despite its reputation as a waste gas, is a critical regulator of oxygen delivery to tissues. Low CO2 causes vasoconstriction and reduces the Bohr effect, paradoxically reducing oxygen availability to the muscles even as ventilation increases.
Trainees with chronic over-breathing often feel breathless during moderate exercise despite having adequate cardiovascular fitness — not because their heart or lungs lack capacity, but because their CO2 regulation is disrupted. Nasal breathing, slower breathing rates, and controlled breath-holding drills gradually restore CO2 tolerance — reducing perceived breathlessness and improving exercise efficiency without any change in cardiovascular fitness.
6 Breathing and Diaphragm Exercises: From Basic to Performance-Integrated
How: Lie on the back, knees bent, one hand on belly, one on chest. Inhale through the nose for 4 seconds — focus on the belly hand rising first and furthest. Chest hand should remain mostly still. Exhale through the mouth for 6 seconds, letting the belly fall. 10 breaths per session, twice daily.
Key point: The 4:6 ratio (inhale shorter than exhale) activates the parasympathetic nervous system. This is not just relaxation — it is deliberate autonomic regulation that resets the chronic sympathetic activation of stress breathing patterns.
Target: Full diaphragmatic excursion, thoracic expansion, rib cage mobility
How: Sit cross-legged or upright. Inhale and direct the breath into the sides and back of the rib cage — not just the front belly. Imagine expanding 360° like a cylinder: front, sides, and back equally. Hold 2 seconds at full expansion. Exhale fully. 8 breaths per set.
Key point: Most trainees only expand the front of the abdomen during diaphragmatic breathing. Posterior and lateral rib cage expansion is what generates maximum intra-abdominal pressure — the component most relevant to spinal stability under load.
How: Lie face down, forehead resting on the back of the hands. Inhale and direct the breath specifically into the back — the lower rib cage should expand laterally and the lower back should rise slightly. Exhale fully. 10 breaths. The prone position restricts anterior belly expansion, forcing the posterior diaphragm to work harder.
Key point: Particularly effective for trainees with dominant anterior breathing. The floor provides biofeedback — you can feel the posterior rib cage expanding against the mat when posterior activation is correct.
🏋️ 4. Bracing Breath (Valsalva Training)
Target: Maximum intra-abdominal pressure, spinal stability under load
How: Stand upright. Take a full diaphragmatic breath into the 360° position. Close the glottis (hold the breath at the throat, not the mouth). Brace the core outward in all directions simultaneously — like bracing for a punch. Hold 3 seconds. Release and breathe out. Practice 5 reps before loading.
Key point: This is the Valsalva in training form. Practising it without load develops the pattern before applying it under a barbell. The quality of the Valsalva under heavy load is only as good as the diaphragmatic breath that precedes it.
How: Use a calibrated inspiratory muscle trainer device (commercially available for £20–60). Inhale forcefully through the device against resistance — the resistance should make inhaling genuinely challenging within 30 breaths. 2 sets of 30 breaths daily, at 50–60% of maximum inspiratory pressure. Increase resistance as the breathing muscles strengthen.
Key point: This is the training method used in the meta-analysis showing improved endurance performance. The device provides calibrated, progressive resistance to the inspiratory muscles — the training stimulus that passive breathing exercises cannot provide for performance development.
🏋️ 6. Box Breathing (Autonomic Reset)
Target: Parasympathetic activation, recovery between hard efforts, pre-performance focus
How: Inhale for 4 counts, hold for 4 counts, exhale for 4 counts, hold for 4 counts. Repeat 4–6 cycles. Use between sets during training to accelerate recovery, before competition to reduce sympathetic arousal, and during cool-down to shift the autonomic state toward recovery mode.
Key point: Box breathing is used by elite military and athletes for performance regulation — not as a relaxation technique but as a deliberate physiological tool. The equal inhale-hold-exhale-hold pattern balances sympathetic and parasympathetic tone more effectively than simple slow breathing.
4-Week Breathing Programme and Common Mistakes
Mistake 1: Practising Only When Lying Down
Most breathing exercises are taught and practised in the supine (lying down) position. Gravity assists diaphragmatic descent in this position — making correct belly breathing easier than in sitting or standing. Trainees who only practise lying down often revert to chest breathing the moment they sit or stand upright, because they never trained the pattern against gravity.
Progression: establish the pattern lying → practise sitting → practise standing → integrate into warm-up and between sets during training. The diaphragmatic breathing pattern only becomes automatic when trained in the positions where it breaks down.
Mistake 2: Forcing the Belly Out
Many trainees interpret “belly breathing” as deliberately pushing the stomach out — using the abdominal muscles to protrude the belly rather than allowing the diaphragm’s descent to naturally displace the abdominal contents outward. This active belly-pushing is not diaphragmatic breathing; it is abdominal wall relaxation.
The correct cue: inhale and let the belly respond to the diaphragm descending. The belly rises as a consequence of diaphragm contraction, not as a deliberate action. The difference is subtle but significant — active belly pushing prevents the intra-abdominal pressure development that makes diaphragmatic breathing valuable for core stability.
Mistake 3: Applying Diaphragmatic Breathing During Maximum Effort
Slow diaphragmatic breathing is inappropriate during maximum lifting efforts. The Valsalva — breath-hold with full brace — is the correct breathing strategy for single heavy reps. Slow diaphragmatic breathing is appropriate for warm-up, recovery between sets, and cool-down.
The goal is to develop the full diaphragmatic capacity that makes a superior Valsalva possible — not to breathe slowly during a maximal deadlift. Confusing these contexts produces either inadequate spinal protection under load or ineffective recovery between efforts.
4-Week Breathing Programme
Perform the breathing exercises daily — 8–10 minutes per session. Progress from supine to upright as each pattern becomes automatic.
📅 Week 1: Foundation — Supine Pattern Establishment
Box breathing 4 cycles before each training session
Focus: Establish belly-first pattern lying down — feel belly hand rising before chest hand
📅 Week 2: Expansion — 360° and Upright Training
360° breathing 2×8 breaths (seated)
Diaphragmatic breathing standing 2×10
Bracing breath practice 3×5 reps (standing, no load)
Box breathing between training sets
Focus: Transfer the pattern to sitting and standing — note if chest takes over when upright
📅 Week 3: Performance Integration
Bracing breath before every heavy working set (deliberate practice)
IMT 2×30 breaths (if device available) OR 360° breathing 3×8
Box breathing during all rest periods between hard sets
Note: does lower back feel more supported under load compared to Week 1?
Focus: Integrate bracing breath into every working set — this is where diaphragm training transfers to training performance
📅 Week 4: Benchmark + Maintenance
Retest supine breathing assessment — which hand moves first now?
Full programme consolidation
Expected outcome: Automatic diaphragmatic breathing in most positions, improved bracing quality under load, reduced upper trap tension, and improved recovery perception between hard training sets.
Maintenance: 5 min of breathing exercises daily — diaphragmatic + 360° + box breathing before training sessions permanently.
Focus: Assess whether the pattern has become automatic — the goal is no longer conscious effort to belly breathe
Frequently Asked Questions About Breathing and Diaphragm Training
How long does it take to change a breathing pattern?
Conscious pattern change — being able to breathe diaphragmatically when deliberately focused — typically occurs within 1–2 weeks of daily practice. Automatic pattern change — diaphragmatic breathing occurring without conscious effort during normal activities — requires 4–8 weeks of consistent training in multiple positions. The transition from conscious to automatic is the meaningful milestone; the breathing exercises in Week 4 assess whether this transition has occurred.
Does diaphragmatic breathing actually improve squat and deadlift performance?
Indirectly — by improving the Valsalva quality that protects the spine and maximises force transfer during heavy lifting. A trainee who previously could not generate adequate intra-abdominal pressure for heavy lifts will notice improved stability and reduced lower back vulnerability after 4–6 weeks of diaphragmatic breathing training. The improvement is not in muscle strength but in the neural coordination that makes existing abdominal and back strength fully accessible under load. See also: core stability guide for how diaphragmatic breathing integrates with the transversus abdominis and pelvic floor in the complete spinal stability system.
Is nasal breathing better than mouth breathing during exercise?
For low and moderate intensity exercise (Zone 1–3), nasal breathing produces several advantages: humidifies and filters inhaled air, maintains optimal blood CO2 levels, and promotes diaphragmatic activation more consistently than mouth breathing. For high-intensity exercise (Zone 4–5) where ventilation demand exceeds nasal capacity, mouth breathing is necessary and appropriate. The practical recommendation: nasal breathe during warm-up, cool-down, and Zone 2 work; switch to mouth breathing when intensity demands it.
Can breathing exercises help with anxiety and stress recovery?
Yes — the autonomic nervous system effects of deliberate breathing are well-established and clinically meaningful. The extended exhale (breathing out longer than you breathe in) activates the vagus nerve and shifts the autonomic state toward parasympathetic dominance. Box breathing and 4:6 breathing ratios produce measurable reductions in cortisol and heart rate variability improvements within a single session. For athletes managing training stress and recovery, breathing practice functions as a practical tool for accelerating the physiological recovery process between hard sessions.
Do I need special equipment for breathing training?
For the foundation and stability work (diaphragmatic, 360°, crocodile, box breathing) — no equipment is needed beyond a mat and attention. For inspiratory muscle training (IMT) — a calibrated breathing resistance device is required (£20–60 commercially). For biofeedback during learning — a simple hand placement (one on belly, one on chest) provides sufficient feedback for establishing the pattern without any additional equipment.
Warning Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. Warning Medical Disclaimer: This article is for general informational purposes only…
You squat, deadlift, and hip thrust consistently. Your glutes still do not look or feel like they are working. Your quads and lower back fatigue first. The glutes seem to sit out. This is not a motivation or effort problem. It is a neuromuscular activation problem. The glutes are the largest and most powerful muscles…
Tight hamstrings are the most commonly cited flexibility limitation in recreational athletes. They are also the most commonly treated incorrectly. The standard approach: stretch the hamstrings for 30 seconds, three times, after training. Sometimes before training. Consistently for a few weeks, then irregularly, then not at all, because nothing seems to change. The hamstrings feel…
The rectus femoris is the quadriceps muscle that crosses two joints rather than one. While the vastus lateralis, vastus medialis, and vastus intermedius cross only the knee, the rectus femoris originates at the anterior inferior iliac spine of the pelvis and crosses both the hip and the knee. This two-joint architecture means the rectus femoris…
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only and does not replace professional medical or fitness advice.If you have chronic lower back pain, spinal pathology, or any musculoskeletal condition — please consult a qualified physiotherapist or healthcare professional before beginning any core stability program. Core stability training has evolved…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. The Fitness Quality Nobody Trains Until It Fails Them Balance is…