
Thoracic Rotation: Why Stiff Mid-Back Rotation Is Destroying Your Shoulder Mobility and Causing Lower Back Pain

Most people who have shoulder pain are told their shoulders are the problem. Most people with lower back pain are told their lower back is the problem. Both diagnoses frequently miss the same contributing factor: restricted thoracic rotation at the mid-back.
The thoracic spine is designed to rotate. It has 12 vertebrae, each with structural features that allow rotation to occur more freely than anywhere else in the spine. When this rotation becomes restricted, typically through prolonged sitting, poor posture habits, or simply a training programme that never takes the thoracic spine through its rotation range, the body redistributes the movement demand to adjacent structures. The shoulder joint compensates by working harder to achieve overhead positions it should reach with help from thoracic rotation. The lumbar spine compensates by rotating when it should not, accumulating stress that contributes to lower back pain.
This guide challenges the common approach of treating shoulder impingement and lower back pain at the site of symptoms, shows what the research demonstrates about thoracic spine involvement in both conditions, explains why conventional stretching often fails to restore thoracic rotation, and provides a targeted protocol specifically for rotation restoration.
The Myth of Treating Shoulder and Back Pain at the Site of Symptoms
Why Symptom-Location Treatment Misses the Source
The assumption underlying most self-directed shoulder and back pain management is that the painful structure is the problem. If the rotator cuff hurts, strengthen the rotator cuff. If the lower back hurts, stretch and strengthen the lower back. This approach addresses the site receiving excess load, not the source of the excessive loading. A rope rubbing against a sharp edge wears fastest at the contact point. The solution is not to strengthen the rope at that point. It is to remove the sharp edge causing the friction.
Restricted thoracic rotation is the sharp edge in many cases of shoulder impingement and lumbar rotation pain. The thoracic spine’s inability to rotate adequately transfers demand to the shoulder during overhead movements and to the lumbar spine during all rotation-requiring activities. The shoulder and lumbar spine are not weak or injured in these cases. They are overloaded by a mobility deficit occurring two to three segments away.
The Thoracic Spine’s Rotation Role and What Restricts It
The thoracic spine normally allows 35 to 50 degrees of rotation to each side, more than any other spinal region. This rotation capacity is structurally built in: the thoracic facet joints are oriented in the frontal plane, favouring rotation over the flexion and extension that the lumbar facets are designed for. When thoracic rotation decreases below its normal range, it does not simply reduce movement at that level. It changes the movement demands at every joint in the kinetic chain that depends on thoracic rotation contribution.
The primary causes of restricted thoracic rotation are prolonged sitting posture with thoracic kyphosis, anterior chest tightness from excessive pressing without thoracic extension work, poor overhead training technique that trains around thoracic stiffness rather than developing thoracic mobility, and general deconditioning of the thoracic rotator muscles. Each cause produces the same result through different pathways: the thoracic vertebrae stop rotating freely, the facet joints stiffen in their resting position, and the compensations above and below the restriction begin accumulating.
The Research: Thoracic Spine Mobility and Rotator Cuff Shoulder Pain
Reduced Thoracic ROM in Shoulder Pain Patients
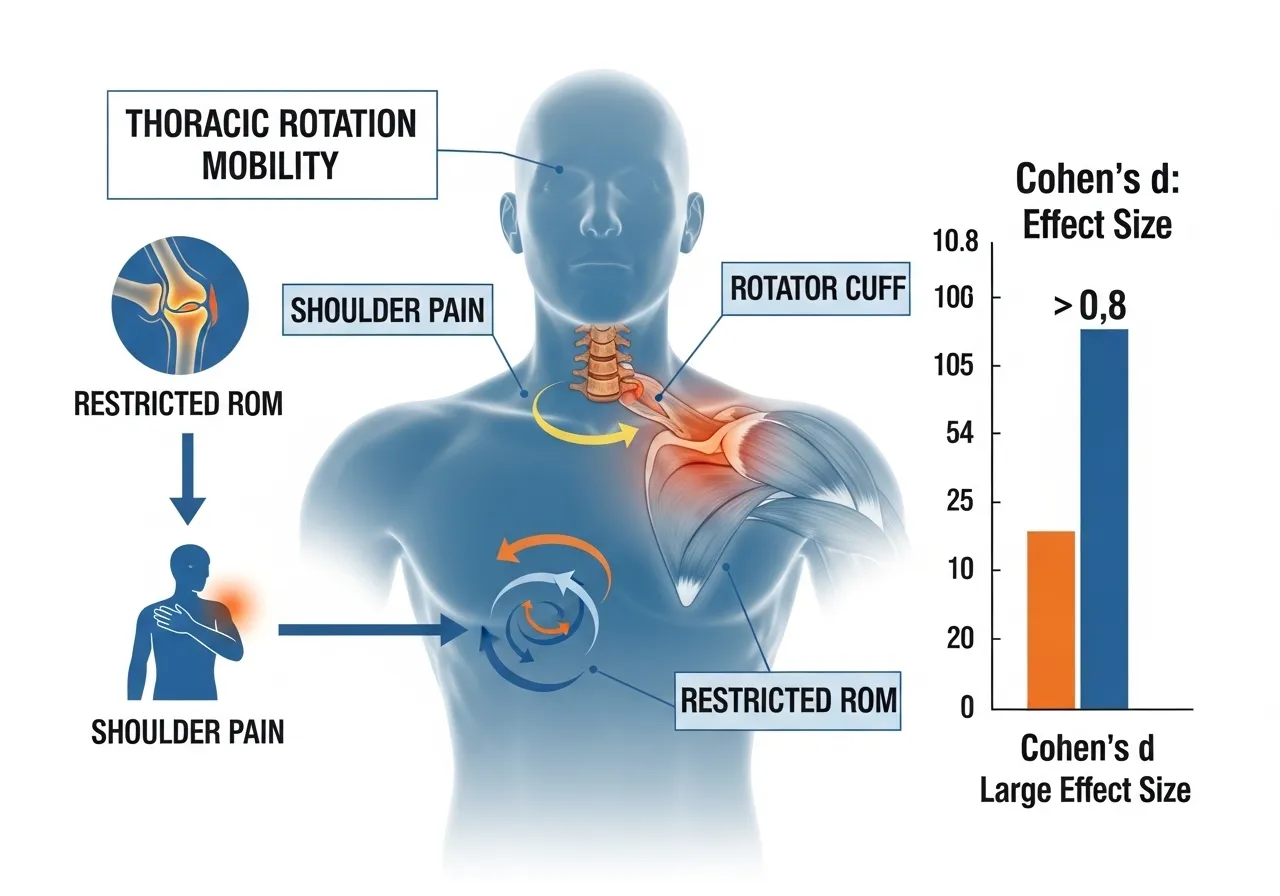
A comparative analysis examining cervical and thoracic spine mobility in patients with rotator cuff related shoulder pain versus asymptomatic controls found that the rotator cuff related shoulder pain group had significantly reduced cervical rotation and flexo-extension range of motion as well as thoracic spine flexion, extension, and rotation compared to asymptomatic controls, with large effect sizes observed for cervical rotation at Cohen’s d of 0.86, cervical flexo-extension at d of 0.80, and thoracic spine flexion at d of 1.04, with the study concluding that cervical and thoracic spine mobility restrictions are clinically relevant findings in rotator cuff related shoulder pain that warrant assessment and treatment as part of comprehensive shoulder pain management.
Shoulder pain patients show significantly restricted thoracic mobility with large effect sizes (Cohen’s d up to 1.04). Thoracic mobility restriction is a clinically relevant finding in shoulder pain warranting direct assessment and treatment, not just rotator cuff strengthening at the symptom site.
Thoracic Rotation and Athletic Injury Risk
Thoracic rotation restrictions link to pathologies in both upper and lower extremities. Treatment guidelines for neck, lower back, shoulder, and elbow pain all include thoracic spine interventions, confirming that thoracic rotation mobility is a shared upstream factor across multiple common musculoskeletal presentations.
Thoracic Mobility Assessment and Shoulder Impingement
A biomechanical and functional analysis comparing shoulder complex and thoracic spine function in patients with subacromial impingement syndrome found that rotator cuff related shoulder pain is a prevalent clinical presentation characterised by substantial diagnostic uncertainty and that some of this uncertainty relates to the involvement of the cervical and thoracic spine as a source of or contributing factor to rotator cuff related shoulder pain, with the comparative analysis showing that thoracic spine mobility assessments provide clinically meaningful information about shoulder pain aetiology beyond what shoulder-specific assessments alone can reveal.
Thoracic spine involvement represents a source of diagnostic uncertainty in shoulder pain. Assessing thoracic mobility alongside shoulder-specific findings provides information about the upstream contributions to shoulder pain that shoulder assessment alone cannot reveal.
How Restricted Thoracic Rotation Specifically Damages the Shoulder and Lower Back
The Shoulder Compensation Mechanism
Overhead pressing, throwing, and swimming all require the arm to reach above shoulder height with the scapula and glenohumeral joint working in coordinated rhythm with thoracic extension and rotation. When the thoracic spine cannot contribute its normal rotation to a throwing or overhead pressing movement, the glenohumeral joint must achieve the required total range of motion alone. This demands greater shoulder external rotation and greater scapular upward rotation than the joint is designed to sustain repetitively under load.
The rotator cuff muscles, particularly the supraspinatus and infraspinatus, work significantly harder to stabilise the humeral head in this compensated overhead position. Over thousands of repetitions, this chronic overload at the rotator cuff produces the tendinopathy and impingement that is then diagnosed and treated as a shoulder problem. The shoulder is where the pain is. The thorax is where the problem originates. Releasing thoracic rotation restriction and including it in shoulder mobility training is covered in the shoulder mobility guide.
The Lumbar Rotation Compensation Mechanism
The lumbar spine is structurally designed to flex and extend, not to rotate. The lumbar facet joints are oriented in the sagittal plane, limiting rotation to approximately 5 degrees per level. The total available lumbar rotation is only 10 to 15 degrees, a fraction of the 35 to 50 degrees available in the thoracic spine.
When thoracic rotation is restricted and a rotation-requiring movement must still occur, the lumbar spine provides compensatory rotation beyond its structural tolerance. Golf swings, throwing mechanics, everyday turning while carrying loads, and rotational athletic movements all demand rotation that should come primarily from the thoracic spine. When it does not, the lumbar facet joints, intervertebral discs, and paraspinal muscles at L4-L5 and L5-S1 absorb the rotation that the thoracic spine refused to provide. This accumulated compensatory lumbar rotation is a primary mechanism behind the lower back pain that responds poorly to direct lumbar treatment but improves with thoracic rotation restoration.
Why Standard Thoracic Stretching Often Fails
The most common approach to thoracic stiffness is foam rolling the thoracic spine in extension over a roller. This addresses thoracic extension restriction, not thoracic rotation restriction. These are different movement planes requiring different interventions. A trainee who foam rolls the thoracic spine diligently every session may develop adequate thoracic extension while the rotation restriction that contributes to their shoulder and lower back problems remains completely unaddressed because rolling in extension does not load the rotational facet mechanics that determine rotation range.
Thoracic rotation requires rotational mobilisation: exercises that take the thoracic vertebrae through their rotation range under load, in positions that isolate thoracic rotation from compensatory lumbar rotation, and with sufficient joint mobilisation to reduce the capsular stiffness that restricts rotation. Extension-based thoracic work remains valuable and is covered in the thoracic mobility guide.
How Do You Know If Thoracic Rotation Is Your Specific Problem?
The Seated Rotation Self-Test
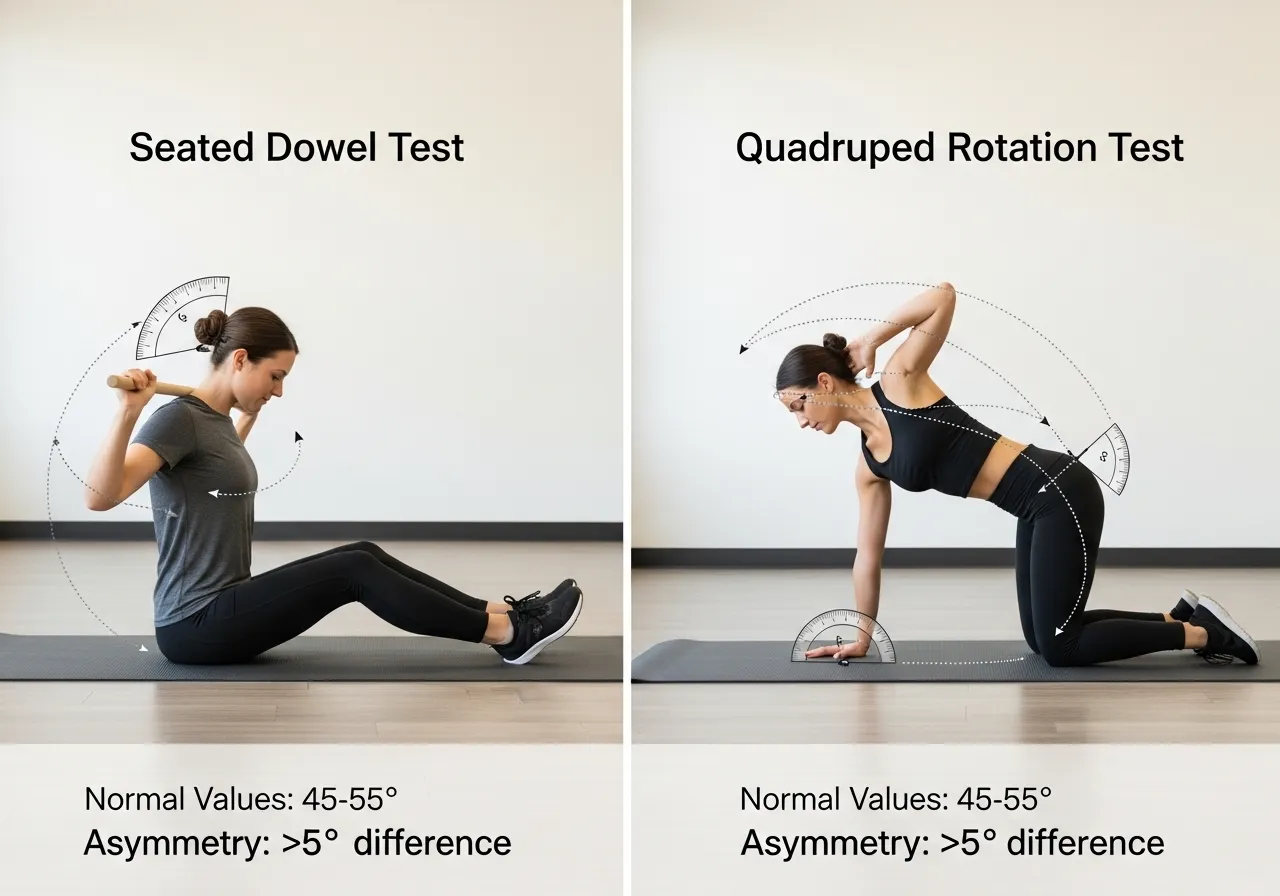
The seated rotation test isolates thoracic rotation from hip and lumbar contribution. Sit on a flat chair with feet flat on the floor and a dowel or broom handle across the shoulders, held with both hands. Cross your arms over the dowel to anchor it. Keep the hips facing forward throughout. Rotate the entire upper body to one side as far as possible without the hips moving. The angle the dowel makes relative to the starting position approximates your available thoracic rotation.
Normal thoracic rotation in the seated position: 40 to 50 degrees per side. A side-to-side difference of more than 10 degrees indicates meaningful rotational asymmetry. Less than 35 degrees on either side indicates restricted thoracic rotation below the range required for normal overhead and rotational movement. If one side is significantly more restricted than the other, sport-specific loading history or habitual posture is likely creating the asymmetry through one-sided rotation demands.
The Quadruped Rotation Test
The quadruped rotation test assesses thoracic rotation with the lumbar spine stabilised by the table-top position. Position on hands and knees with hands under shoulders and knees under hips. Place one hand behind the head with the elbow pointing outward. Rotate the upper body to lift that elbow toward the ceiling while keeping the opposite hand on the floor and the hips square. The ceiling-facing elbow angle approximates available thoracic rotation in this position.
This test is more functionally relevant than the seated test because the quadruped position prevents lumbar rotation compensation, revealing the thoracic rotation available without the lumbar cheating that the seated test can allow. Normal range is approximately 50 to 60 degrees of elbow elevation. Consistent restriction to less than 40 degrees on either side, or marked asymmetry between sides, identifies thoracic rotation restriction requiring direct intervention.
Differentiating Rotation Restriction from Extension Restriction
Thoracic extension restriction and thoracic rotation restriction frequently co-exist but can be present independently. A trainee with adequate thoracic extension but restricted rotation will show normal foam roller response but poor seated rotation test results. A trainee with primary extension restriction but adequate rotation shows the reverse pattern. The distinction matters because they require different exercises and because addressing only extension while rotation remains restricted leaves the compensation mechanisms intact. Assess both dimensions before designing any thoracic mobility intervention.

The 7 Most Effective Thoracic Rotation Exercises
🔄 1. Quadruped Thoracic Rotation
Target: Thoracic rotation with lumbar stabilised, primary rotation drill
How: Hands and knees, table-top position. One hand behind head. Rotate the upper body to lift the elbow toward the ceiling, following with the eyes. Pause 1 to 2 seconds at end range. Return. Perform 8 to 10 slow repetitions per side.
Key point: Keep the hips square throughout. Any hip rotation is lumbar compensation. Slow the movement down to ensure the rotation comes from the thoracic vertebrae, not from momentum or hip drive.
🔄 2. Open Book Rotation (Side Lying)
Target: Thoracic rotation combined with chest opening, posterior capsule stretch
How: Lie on one side with both knees bent to 90 degrees and hips at 90 degrees. Both arms extended in front, palms together. Rotate the top arm backward toward the floor behind you, following with the head and eyes. Allow the chest to open toward the ceiling. Hold 2 to 3 seconds at end range. Return.
Key point: The top knee stays on the floor or on a pillow between the knees throughout. Allowing the knee to lift converts the movement to a hip and lumbar rotation stretch rather than thoracic rotation.
🔄 3. Seated Thoracic Rotation with Dowel
Target: Functional rotation range in the position most relevant to daily life and overhead training
How: Sit upright on a chair. Place a dowel across the shoulders, arms crossed over it. Keeping hips forward, rotate the upper body to one side to end range. Add 3 to 5 small oscillatory movements at end range to load the joint at its limit. Return and repeat to the other side.
Key point: The oscillatory movements at end range provide a gentle joint mobilisation stimulus that sustained stretching does not produce. Perform them with low force but deliberate intent to push the rotation range slightly beyond the passive end range.
🔄 4. Thoracic Rotation with Hip Lock (Kneeling)
Target: Isolated thoracic rotation with pelvis completely fixed
How: Kneel with one knee up and the opposite knee down (half-kneeling position). Place a stick or dowel vertically in front of the down knee, touching it to prevent it from moving. Place both hands behind the head and rotate toward the up-knee side. The down-knee side resistance isolates the rotation to the thoracic spine.
Key point: The most demanding thoracic rotation isolation exercise in the series. Appropriate after basic quadruped and open book work has established some rotation range.
🔄 5. Thread the Needle
Target: Thoracic rotation under gravity, passive end-range loading
How: Hands and knees position. Slide one arm along the floor underneath the body, rotating the shoulder toward the floor on that side. The arm threads through the space between the supporting arm and knee. Hold 15 to 20 seconds at the deepest rotation point. Return. Perform 3 to 5 reps per side.
Key point: The long hold allows gravity to provide a gentle sustained rotational stretch. Useful as a warm-up before training and as a recovery tool between heavy pressing sessions.
🔄 6. Thoracic Rotation CARs (Controlled Articular Rotations)
Target: Active control through the full rotation range, joint health under muscular load
How: Standing or seated. Cross arms over the chest. Initiate a deliberate, maximally controlled thoracic rotation to one side with no momentum. Maintain tension throughout the range, as if pressing against resistance in both directions. Pause at end range, then return with the same deliberate control. Perform 5 to 8 reps per side.
Key point: CARs develop active rotation control, not just passive range. The deliberate tension throughout the movement trains the thoracic rotator muscles through their full range, developing the active mobility that transfers to overhead pressing and rotation-based athletic movements.
🔄 7. Rotation with Overhead Reach Integration
Target: Functional transfer of thoracic rotation to overhead movement patterns
How: From a deep squat or standing position, reach one arm overhead while rotating the thoracic spine toward that arm. The rotation and overhead reach occur simultaneously, integrating the thoracic rotation range into an overhead position. Perform 8 to 10 reps per side.
Key point: This is the integration drill that transfers isolated thoracic rotation work into the combined pattern that overhead pressing and throwing require. Include it at the end of every thoracic rotation session to begin bridging isolated mobility gains to functional movement.
6-Week Thoracic Rotation Restoration Protocol
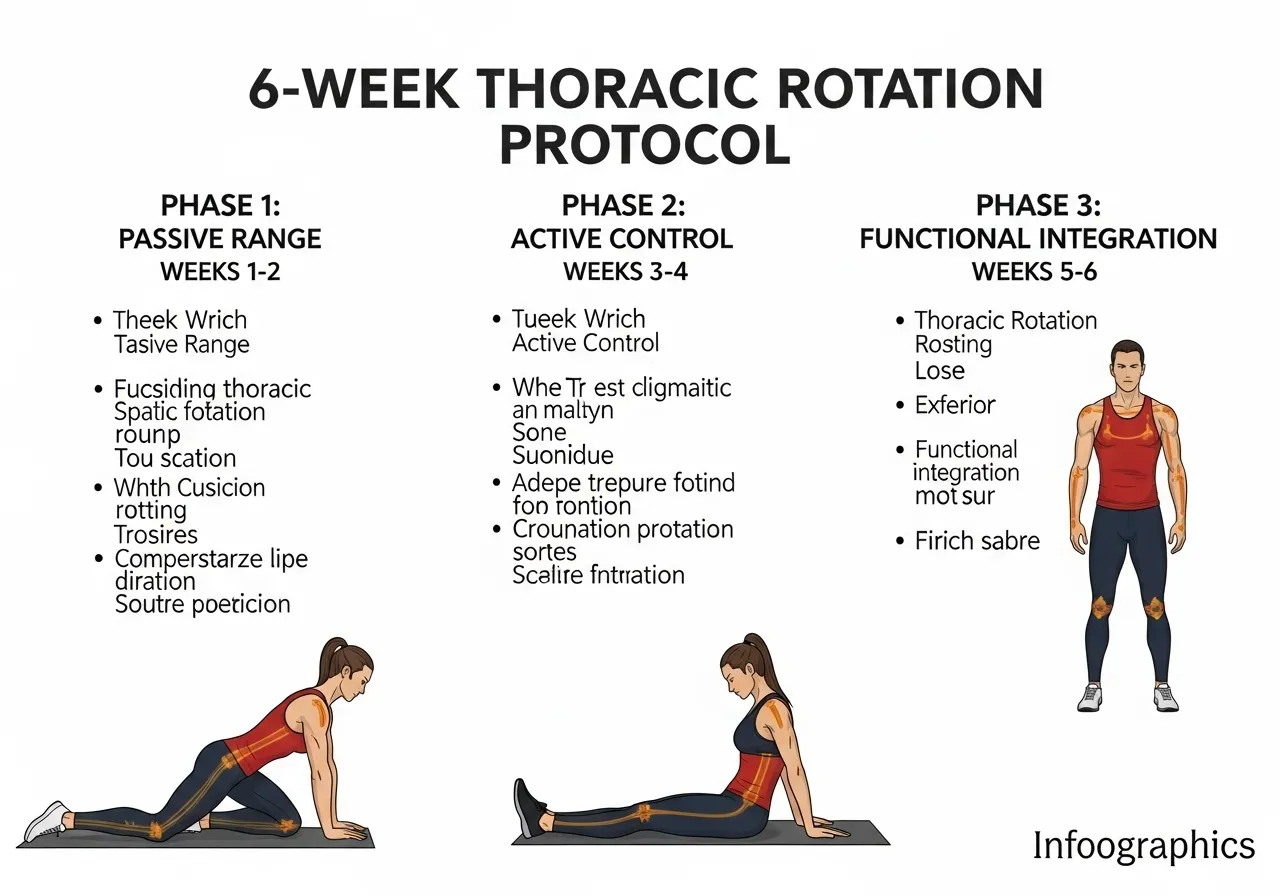
📅 Phase 1: Weeks 1 to 2: Baseline and Passive Range Development
- Perform seated rotation and quadruped rotation tests to establish baseline and side asymmetry
- Open book rotation: 3 sets of 10 reps per side, daily
- Thread the needle: 3 sets of 5 reps per side (15-second holds), daily
- Quadruped thoracic rotation: 3 sets of 8 reps per side, daily
- Focus: identify the more restricted side and note shoulder and back symptom response
Daily frequency is essential in Phase 1. The joint capsule stiffness that restricts thoracic rotation requires daily loading to begin changing. Twice-weekly work at this stage produces minimal progress.
📅 Phase 2: Weeks 3 to 4: Active Control Development
- Continue Phase 1 exercises daily at reduced volume (2 sets each)
- Add seated rotation with dowel and oscillatory end-range work: 3 sets of 12 reps per side
- Add thoracic rotation CARs: 2 sets of 8 reps per side, before every training session
- More restricted side receives one additional set per exercise
Phase 2 converts passive range gains into active control. The CARs before training sessions begin integrating the improved rotation range into the nervous system’s active movement patterns.
📅 Phase 3: Weeks 5 to 6: Functional Integration
- Maintain Phase 2 work at reduced frequency (5 days per week)
- Add kneeling hip-lock rotation: 3 sets of 8 reps per side
- Add rotation with overhead reach integration: 3 sets of 10 reps per side
- Week 6: retest seated and quadruped rotation, compare to baseline
- Expected: 8 to 15 degree improvement in the restricted direction
Phase 3 transfers isolated rotation gains into the functional overhead pattern. The overhead integration drill bridges the gap between mobility in isolation and mobility under the compound demands of pressing and athletic movement.
Programming Thoracic Rotation Work Into Your Training Week
When to Do Thoracic Rotation Work
Thoracic rotation work is most effective as a training session warm-up rather than as a separate mobility session. Performing 5 to 8 minutes of thoracic rotation exercises before overhead pressing, rowing, or rotational sport training prepares the thoracic spine for the rotation demands of the session and reduces the compensatory loading on the shoulder and lumbar spine during the actual training work.
Including 2 to 3 thoracic rotation exercises before every strength session costs minimal time but ensures the thoracic spine enters each session in the most mobile state possible. The shoulder mobility work that pairs with thoracic rotation preparation for comprehensive overhead movement readiness is covered in the shoulder mobility guide.
Daily vs Session-Based Work
During an active restoration phase (the first 4 to 6 weeks addressing established restriction), daily thoracic rotation work produces significantly faster improvement than session-based work alone. The capsular stiffness that restricts rotation requires frequent loading to begin remodelling. Once baseline rotation range is established and maintained, transitioning to session-based work as a warm-up is sufficient to prevent regression.
The distinction matters for time management. A trainee addressing active restriction should prioritise daily 8 to 10 minutes of rotation work above other optional mobility work during the restoration phase. A trainee maintaining adequate rotation should include 3 to 5 minutes of rotation warm-up before each relevant session rather than dedicating separate daily sessions to maintenance.
Connecting Thoracic Rotation to Ankle Mobility in the Full Kinetic Chain
The thoracic spine’s rotation restriction often accompanies ankle dorsiflexion restriction in the same training population. Both restrictions share the same root cause: prolonged sitting produces hip flexor shortening, thoracic flexion and rotation restriction, and reduced ankle range from sustained plantar flexion in seated postures. Trainees addressing thoracic rotation frequently discover that ankle dorsiflexion restriction is a simultaneous limitation. The ankle mobility mechanics and how restricted dorsiflexion contributes to the same squat and overhead compensations that thoracic restriction produces is covered in the ankle mobility guide.
Frequently Asked Questions About Thoracic Rotation Mobility
How quickly does thoracic rotation improve with consistent work?
Initial improvements in thoracic rotation range from daily targeted work appear within 1 to 2 weeks. These early gains reflect primarily neurological changes, reduced protective muscle guarding around stiff segments, rather than structural capsular change. Structural improvement in joint capsule extensibility requires 4 to 6 weeks of consistent daily work.
Trainees who have had restricted thoracic rotation for years, typically those with longstanding desk-based posture habits, require longer restoration timelines than those whose restriction developed over months. Chronic restriction involves greater tissue adaptation and requires more consistent intervention before meaningful range change occurs. Realistic expectations for established restriction: noticeable improvement within 2 weeks, meaningful functional change within 4 to 6 weeks, full restoration in 8 to 12 weeks for significant longstanding restriction.
Should I see a physiotherapist for thoracic rotation restriction?
Mild to moderate thoracic rotation restriction without associated arm pain, nerve symptoms, or severe functional limitation responds well to the self-directed protocol described in this guide. Daily targeted rotation work with the exercises above produces improvement in most cases of non-pathological restriction.
Seek physiotherapist assessment if restriction is accompanied by radiating arm pain or numbness, if one-sided restriction developed suddenly without clear postural cause, if thoracic rotation work consistently produces pain rather than stretch sensation, or if 6 weeks of consistent daily work produces no improvement. These presentations suggest structural pathology or nerve involvement that requires clinical assessment before continuing self-directed mobility work.
Can thoracic rotation restriction cause headaches?
Upper thoracic rotation restriction at T1 to T4 can contribute to cervicogenic headaches through its mechanical effect on the cervical spine. The upper thoracic segments are directly connected to the lower cervical segments through both joint articulations and shared muscle attachments. When upper thoracic rotation is restricted, the cervical spine compensates by increasing its own rotation contribution, creating sustained mechanical load at C5-C6 and C6-C7 that contributes to the cervicogenic headache pattern.
Trainees with frequent cervicogenic headaches who have not specifically addressed upper thoracic rotation often report headache frequency reduction after 4 to 6 weeks of consistent thoracic rotation work. The upper thoracic focus of the seated rotation with dowel exercise and the open book rotation specifically mobilises the segments most relevant to this cervicogenic pattern.
- Shoulder pain and lower back pain patients show significantly restricted thoracic mobility with large effect sizes. Thoracic restriction is a source of upstream loading that creates symptoms at distant structures, not just a local finding.
- Thoracic rotation restriction forces the glenohumeral joint to compensate during overhead movement and the lumbar spine to rotate beyond its structural tolerance, generating both rotator cuff overload and lumbar rotation pain.
- Standard foam rolling in extension does not address rotation restriction. Thoracic rotation requires rotational mobilisation in positions that isolate thoracic rotation from lumbar compensation.
- Daily frequency is essential during active restoration. The joint capsule stiffness driving rotation restriction requires daily loading to remodel. Twice-weekly work produces minimal progress in established restriction.
- Active rotation control through thoracic CARs and integration drills is necessary to transfer mobility gains to functional overhead and rotational athletic movement. Passive range without active control does not change loading patterns under training demands.











