
Nerve Flossing: The Neural Mobilisation Technique That Relieves Sciatica, Radiating Arm Pain, and Neural Tension
Sciatica is one of the most common causes of persistent lower body pain in active adults, and radiating arm pain from cervical nerve compression is its upper body equivalent. Both conditions share a mechanism: the peripheral nerve is irritated, compressed, or has lost its normal ability to glide freely through the surrounding tissues. Movement that should be pain-free produces sharp, burning, or shooting pain because the nerve is being stretched or compressed against a structure it cannot move away from.
Nerve flossing, also called neural mobilisation or neurodynamic exercise, is a movement technique that mobilises peripheral nerves by creating a longitudinal gliding motion of the nerve through its surrounding tissue tunnel. Rather than stretching the nerve to its limit and holding, as conventional stretching does with muscles, nerve flossing uses alternating end-range positions that create a pumping or sliding action along the nerve’s path. The nerve moves through the tunnel; the surrounding structures create and release tension rhythmically.
This guide covers what nerve flossing is, how it differs from conventional stretching, what the systematic review and meta-analysis evidence shows about its effectiveness for sciatica and radicular pain, the two fundamental techniques (slider and tensioner), specific protocols for the sciatic nerve and median nerve, and the safety considerations that determine when to use each approach.
What Is Nerve Flossing and How Does It Differ From Stretching?
The Nerve as a Dynamic Structure
Peripheral nerves are not passive conduits for electrical signals. They are dynamic mechanical structures that must glide, stretch, and compress in coordination with the joints and muscles they pass through during movement. The sciatic nerve, for example, must accommodate several centimetres of longitudinal movement as the hip flexes and the knee extends during a straight leg raise. The median nerve must glide through the carpal tunnel as the wrist moves through its full range. When this normal neural mobility is restricted, movement creates pain not in the muscle but along the nerve’s path.
Neural mobility restriction occurs through several mechanisms: scar tissue formation around the nerve from previous injury or surgery, compression from adjacent structures such as a herniated disc or inflamed muscle pressing on the nerve, increased neural tissue sensitivity from inflammation that lowers the threshold for pain during mechanical loading, and sustained positions that place the nerve under continuous tension without the intermittent decompression that normal movement provides. Each mechanism responds differently to treatment, but all can be addressed to varying degrees through neurodynamic exercise.
Slider vs Tensioner: The Two Fundamental Techniques
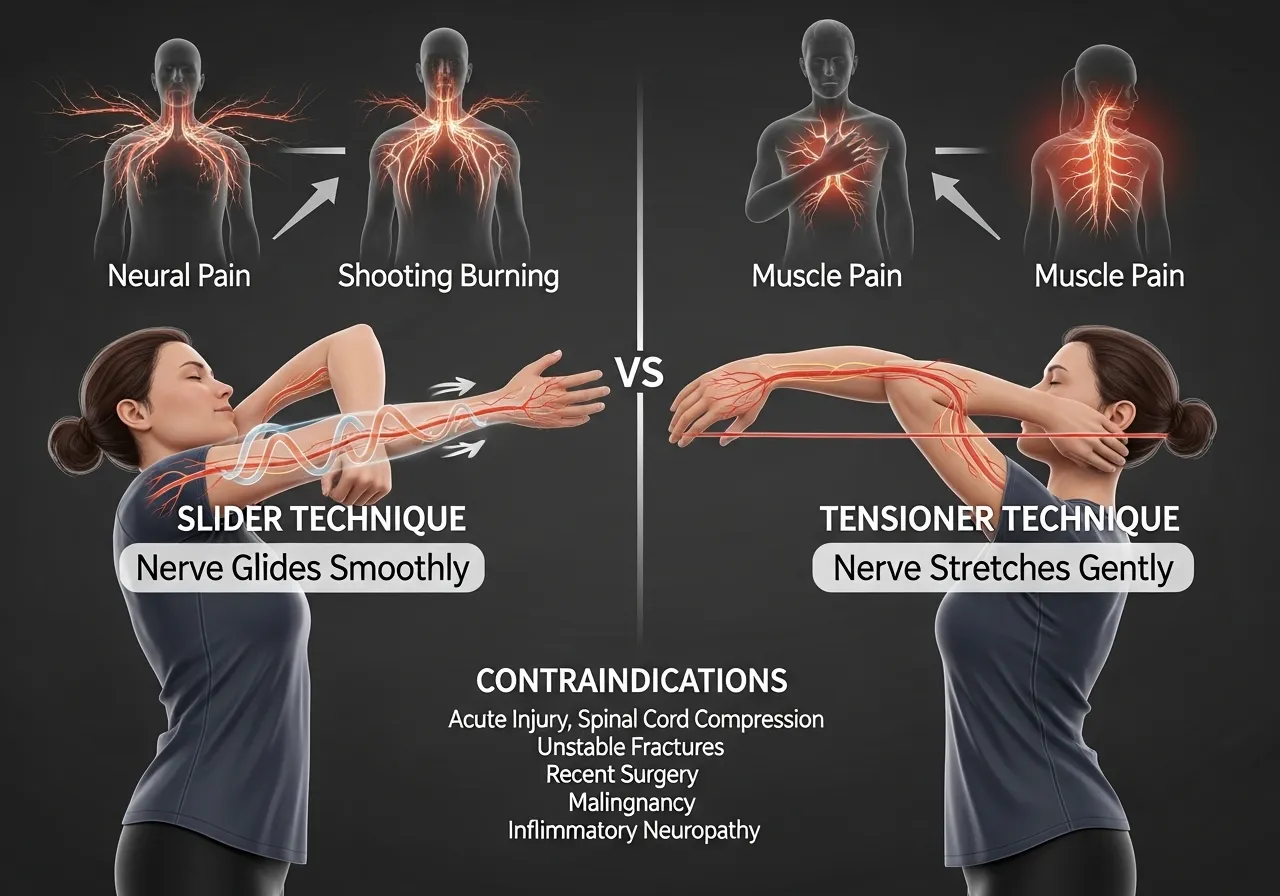
Neural mobilisation uses two fundamentally different mechanical approaches. The slider technique creates longitudinal nerve movement by alternating joint positions at opposite ends of the nerve, so that as one end increases tension on the nerve, the other end releases it. The nerve slides back and forth through its tunnel without the net tension increasing. The tensioner technique moves both ends of the nerve simultaneously into positions that increase neural tension, creating a sustained stretch on the nerve tissue itself.
The distinction matters clinically. Sliders produce greater longitudinal nerve excursion (movement through the tunnel) with less peak neural tension at each end of the movement. They are appropriate for acutely irritated nerves where any significant tension increase would provoke severe symptom aggravation. Tensioners produce greater neural tension and less longitudinal excursion. They are appropriate for less sensitive presentations where the goal is increasing the nerve’s tolerance to tension rather than simply improving its gliding capacity.
Why Nerve Flossing Works: The Proposed Mechanisms
Several mechanisms explain why neural mobilisation reduces neural pain and improves function. Fluid dynamics: the repeated gliding motion creates a pumping effect within the neural sheath that disperses inflammatory mediators and oedema that accumulate in compressed or sensitised neural tissue. Axonal transport: longitudinal nerve movement improves the transport of proteins and nutrients along the axon that sustains neural tissue health. Mechanical desensitisation: repeated submaximal mechanical loading of sensitised neural tissue gradually reduces the central sensitisation that makes the nerve hypersensitive to normal mechanical stimuli. Adhesion release: in cases where scar tissue or adhesions restrict neural gliding, the repeated movement gradually increases the mechanical freedom of the nerve within its tunnel.
When Nerve Flossing Is Not Appropriate
Neural mobilisation is contraindicated or requires modification in several clinical presentations. Active nerve root compression with significant neurological deficit (weakness, loss of reflexes, bowel or bladder changes) requires medical assessment before any neurodynamic exercise. Severe acute sciatica where any leg movement produces severe radiating pain below the knee warrants a brief acute management period before progressive neural mobilisation is introduced. Cauda equina syndrome, a medical emergency, must be excluded before any lower limb neural mobilisation is attempted in someone with new onset bilateral leg symptoms or bladder and bowel changes.
The Difference Between Neural Pain and Muscle Pain
Identifying neural tension as the source of symptoms rather than muscle tightness determines whether nerve flossing is the appropriate intervention. Neural pain has characteristic features that distinguish it from muscular pain: it follows a consistent anatomical pathway rather than diffusing broadly, it often has a sharp, burning, shooting, or electric quality rather than the dull aching of muscle discomfort, it is frequently provoked by specific positions that tension the nerve (sitting for prolonged periods in sciatica, reaching overhead in cervical radiculopathy), and it may be accompanied by numbness, tingling, or sensitivity changes along the nerve’s distribution. When these features are present, neurodynamic exercise rather than conventional stretching is the appropriate primary intervention.
The Research: What Meta-Analyses Show About Neural Mobilisation Effectiveness
Neural Mobilisation for Lumbar Radiculopathy: Meta-Analysis Evidence
A systematic review and meta-analysis examining neural mobilisation for reducing pain and disability in patients with lumbar radiculopathy found that the most commonly studied technique was neural mobilisation and most studies reported significant improvement in the outcomes, with the meta-analysis providing evidence that neural mobilisation techniques can alleviate pain and reduce disability in patients with lumbar radiculopathy, demonstrating clinically meaningful reductions in pain intensity and disability scores across the included randomised controlled trials, and confirming that neural mobilisation represents an effective non-surgical intervention for the management of radicular lower limb pain from lumbar nerve compression.
Neural mobilisation produces clinically meaningful reductions in pain and disability in lumbar radiculopathy. The technique is supported by multiple RCTs as an effective non-surgical intervention for sciatica and lower limb radicular pain.
Neural Mobilisation for Broader Musculoskeletal Pain: Systematic Review
A systematic review with meta-analysis examining neural mobilisation across musculoskeletal pain conditions found that neural mobilisation techniques produced improvements in pain intensity, functional status, and physical performance in adults with musculoskeletal pain, with the evidence indicating that neurodynamic techniques applied to peripheral nerves produce measurable outcomes across a range of pain presentations beyond specifically radicular conditions, and that the techniques appear safe and producible across different clinical populations when applied with appropriate load management.
Neural mobilisation improves pain, function, and physical performance across a range of musculoskeletal conditions. The benefits extend beyond sciatica to carpal tunnel syndrome, cervical radiculopathy, plantar fasciitis with neural involvement, and other peripheral nerve compression presentations.
Slider vs Tensioner: What the Comparison Evidence Shows
A prospective controlled trial comparing slider and tensioner neurodynamic exercises in patients with low back-related leg pain and peripheral nerve sensitisation found that both slider and tensioner techniques produced short-term improvements in pain and straight leg raise range of motion in peripheral nerve sensitisation presentations. The slider technique produced these improvements with lower symptom provocation during treatment, while the tensioner technique produced slightly greater gains in neural tension tolerance at the cost of more treatment-session discomfort. This comparison confirms that slider technique is the appropriate starting point for acutely sensitised presentations, with tensioner introduction as tolerance improves.
The Nerve Flossing Evidence for Athletes and Active Individuals
Research specifically examining neural mobilisation in active populations, including athletes and physically active adults, consistently shows that neurodynamic exercises are an effective adjunct to standard training for individuals experiencing neural tension-related symptoms. Athletes who develop sciatic symptoms from prolonged sitting, repetitive hip flexion loading, or piriformis irritation typically respond well to sciatic nerve slider exercises performed daily or twice daily, with symptom improvement appearing within 1 to 2 weeks in acute presentations and 3 to 6 weeks in chronic cases.
The evidence for nerve flossing as a preventive technique for neural tension management before symptom onset in high-risk activities such as prolonged computer work, cycling at aggressive positions, or sport activities requiring repeated hip flexion combined with knee extension shows that neurodynamic tension techniques used as prophylactic treatment produced measurable effects on neural tension and nerve excursion, suggesting that the technique has potential preventive applications beyond its established therapeutic role in symptomatic radiculopathy.
Neurodynamic tension techniques show potential as preventive treatments for neural tension accumulation in high-risk activities, not only as therapeutic interventions for established radicular pain.
How Quickly Does Nerve Flossing Work?
Acute neural tension symptoms typically show measurable improvement within the first 3 to 7 days of consistent twice-daily nerve flossing. The early improvement reflects primarily the fluid dynamics mechanism: inflammatory mediators are dispersed and neural oedema reduces, lowering the nerve’s mechanical sensitivity without substantial structural change. Structural improvements in neural gliding capacity and reduction of adhesion-related restriction require 3 to 6 weeks of consistent work in chronic presentations. Most individuals notice reduced symptom provocation with the straight leg raise or upper limb tension tests within the first week of appropriate technique use if the neural technique is correctly matched to the presentation.
Sciatic Nerve Flossing: The 4 Most Effective Techniques
The Sciatic Nerve Anatomy: Why the Technique Must Address Two Joints
The sciatic nerve exits the lumbar spine, passes through the piriformis region of the posterior hip, travels down the posterior thigh, and branches at the knee into the tibial and common peroneal nerves. It crosses two major joints (hip and knee) and is influenced by the ankle position as well. Effective sciatic nerve flossing must create longitudinal movement of the nerve by manipulating these joints in coordinated sequences, not by simply stretching the hamstrings or piriformis in isolation.
🔄 1. Supine Sciatic Slider (Seated Slump Variation)
Target: Sciatic nerve gliding through the posterior chain from ankle to lower back
How: Lie on the back with both knees bent to 90 degrees. Bring one knee to the chest. Simultaneously: extend the knee to straighten the leg while plantarflexing the ankle (pointing the foot), then flex the knee back while dorsiflexing the ankle (pulling toes toward shin). The plantarflexion-with-knee-extension and dorsiflexion-with-knee-flexion alternation creates the slider motion. Perform 10 to 15 slow repetitions.
Key point: This is the gentlest sciatic slider technique and the appropriate starting point for acutely irritated sciatica. Symptoms should not increase during or after the technique. If radiating pain below the knee worsens, reduce the range of knee extension.
🔄 2. Seated Sciatic Slider (Neural Slump Technique)
Target: Sciatic nerve with cervical spine contribution, more complete neural chain
How: Sit on the edge of a chair with upright posture. Simultaneously: extend one knee to straighten the leg and flex the neck (chin toward chest), then flex the knee and extend the neck (look up). The neck and knee move in opposite directions simultaneously. This couples cervical flexion with knee extension to create greater neural chain loading and release. Perform 10 to 15 repetitions.
Key point: The cervical component of this technique means it mobilises the entire neural chain from neck to foot simultaneously. It is more provocative than the supine version and should be introduced only after the supine slider is tolerated without symptom increase.
🔄 3. Standing Sciatic Slider
Target: Sciatic nerve in functional standing position, more load than supine
How: Stand with hands on a wall or chair back for balance. Flex the hip to 70 to 80 degrees (thigh near horizontal). Alternately extend and flex the knee while keeping the hip angle fixed. The knee extension stretches the sciatic nerve; the knee flexion releases it. Perform 10 to 15 repetitions per side.
Key point: The standing position adds body weight load to the neural glide. Appropriate for sub-acute and chronic presentations where the supine slider is well tolerated and more functional loading is appropriate.
🔄 4. Sciatic Tensioner (Advanced)
Target: Maximum sciatic nerve tension load, tolerance development
How: Perform the seated slump technique but hold both ends of the neural chain at end range simultaneously: knee extended, ankle dorsiflexed, and neck flexed. Hold 3 to 5 seconds, then release all positions simultaneously. This creates sustained neural tension rather than the dynamic gliding of the slider techniques. Perform 5 to 8 repetitions per side.
Key point: Tensioner techniques produce more discomfort than sliders because they sustain neural tension rather than cycling it. Appropriate for chronic, less sensitive presentations where the goal is neural tension tolerance development rather than symptom reduction from acute irritation.
Progressing From Slider to Tensioner
The progression from slider to tensioner techniques should follow symptom response rather than time elapsed. When slider exercises consistently produce no symptom provocation during or after the session, and when the straight leg raise range has improved to within 10 to 15 degrees of the non-affected side, tensioner introduction is appropriate. If any tensioner technique produces marked symptom increase lasting more than 30 minutes after the session, return to slider technique and progress more gradually.

Median Nerve Flossing for Arm Pain, Carpal Tunnel, and Cervical Radiculopathy
The Median Nerve Anatomy and Upper Limb Neural Tension
The median nerve exits the lower cervical and upper thoracic spine, passes through the brachial plexus at the shoulder, travels down the anterior forearm, and passes through the carpal tunnel at the wrist. It provides sensation to the thumb, index, and middle fingers and motor control to the thenar muscles of the hand. Neural tension along this path produces the burning, tingling, or numbness in the hand and forearm that characterises carpal tunnel syndrome, pronator teres syndrome, and cervical C6 or C7 radiculopathy.
Upper Limb Tension Test: The Assessment That Guides Treatment
Before beginning median nerve flossing, the upper limb tension test (ULTT1) identifies whether median nerve tension is the source of upper limb symptoms. Extend the arm at 90 degrees from the body. Extend the elbow and wrist, externally rotate the shoulder, and extend the fingers. Gently add cervical lateral flexion away from the tested arm. If this position reproduces the arm or hand symptoms (not just discomfort in the shoulder or upper arm), median nerve tension is contributing to the presentation and neurodynamic exercise is appropriate.
Median Nerve Slider Technique
The median nerve slider uses opposite movements at the wrist and neck to create a nerve-gliding motion. Extend the wrist (palm facing up, fingers extended) while flexing the neck toward the same shoulder. Then flex the wrist (palm closed, fingers curled) while extending the neck away from that shoulder. These opposite joint movements create the sliding motion at the nerve without building sustained neural tension. Perform 10 to 15 slow repetitions on the symptomatic side.
Median Nerve Tensioner for Carpal Tunnel and Forearm Symptoms
The median nerve tensioner creates sustained tension by positioning the arm, wrist, and fingers in the position that maximally stretches the nerve simultaneously. Extend the elbow fully, extend the wrist to end range, extend all fingers, and externally rotate the shoulder. Hold 3 to 5 seconds. Return all positions to neutral simultaneously. This technique specifically targets carpal tunnel neural tension and is the most effective neurodynamic approach for early to moderate carpal tunnel syndrome symptoms where the nerve remains mobile but sensitised.
When to Seek Assessment Rather Than Self-Treat
Nerve flossing is appropriate for self-directed use in mild to moderate neural tension presentations with confirmed neural involvement through clinical tests. Seek physiotherapist or medical assessment before beginning nerve flossing if: symptoms are severe or rapidly worsening, neurological deficits are present (weakness, lost reflexes, bowel or bladder changes), symptoms are bilateral in both legs or both arms simultaneously, the presentation includes cervical or lumbar pain with any signs of spinal cord involvement, or symptom aggravation after attempted nerve flossing persists beyond 1 hour. The thoracic rotation restriction that commonly accompanies cervical neural tension presentations is addressed in the thoracic rotation guide.
Integrating Nerve Flossing With Strengthening
Neural mobilisation addresses the mobility and sensitivity of the nerve. The underlying mechanical reason for the neural tension, whether it is piriformis compression on the sciatic nerve, carpal tunnel narrowing from flexor tendon swelling, or disc herniation irritating a nerve root, also requires attention. For many trainees, the neural tension that produces sciatica occurs in the context of hip muscle imbalances that create piriformis overload. Addressing hip abductor and deep external rotator weakness through targeted strengthening reduces the piriformis compression that sensitises the sciatic nerve, producing more durable relief than nerve flossing alone can provide without the underlying muscle balance intervention. The quadratus lumborum tightness that contributes to the same lower back and gluteal tension is addressed in the QL guide.
Nerve Flossing Protocols: Daily Practice for Sciatic and Upper Limb Presentations
Frequency and Dosage: The Research-Supported Approach
Neural mobilisation research consistently supports twice-daily application for acute and subacute presentations, with once-daily maintenance appropriate once symptoms are controlled. Each session requires only 5 to 10 minutes for a complete protocol because the treatment effect comes from repeated gentle movement rather than prolonged sustained positions. The neural pumping mechanism that disperses inflammatory mediators is most effective with moderate repetition counts of 10 to 15 reps performed smoothly and without forcing range, rather than fewer repetitions held at end range.
📅 Acute Sciatica Protocol (Weeks 1 to 2)
- Supine sciatic slider only (the gentlest technique)
- 10 to 15 repetitions per session, twice daily (morning and evening)
- Range limited to pain-free knee extension (do not push into radiating leg pain)
- No tensioner techniques at this stage
- Combine with anti-inflammatory position management: avoid prolonged sitting
The gentle supine slider disperses neural oedema and begins restoring neural glide without provoking the acute neural sensitivity that more aggressive techniques would aggravate. Expect gradual improvement in straight leg raise range and reduction in radiating pain intensity within the first 5 to 7 days.
📅 Subacute Protocol (Weeks 3 to 4)
- Progress to seated sciatic slider if supine version is tolerated without symptom increase
- 15 repetitions per session, twice daily
- Introduce standing slider at end of week 3 if seated version is comfortable
- Begin lumbar and hip strengthening to address underlying muscle imbalance
The progression from supine to seated to standing reflects both increasing neural load and increasing functional relevance. Standing slider in week 3 or 4 bridges the gap between protected neural mobilisation and return to full activity loading.
📅 Chronic Management Protocol (Ongoing)
- Once daily maintenance: 10 to 15 reps of preferred slider technique
- Introduce tensioner technique 2 to 3 times per week for tolerance development
- Perform before activities known to provoke neural symptoms (long driving, cycling, sitting)
- Integrate with hip mobility work for sustained neural mobility maintenance
Chronic neural tension requires ongoing management rather than a fixed treatment period. The hip mobility work that addresses the underlying hip tissue restrictions that contribute to chronic sciatic nerve tension is covered in the hip mobility guide.
The Response Rule: How to Know If the Technique Is Working
Neural mobilisation should produce one of three acceptable responses: symptoms stay the same during the session and improve gradually across days (good), symptoms transiently increase during the technique but return to baseline within 30 minutes (acceptable), or symptoms are unchanged by the technique in either direction (appropriate to progress or seek assessment). An unacceptable response is symptoms that worsen during the technique and do not return to baseline within 30 minutes of completing the session. Any worsening response that persists beyond 30 minutes indicates either incorrect technique selection, excessive range or intensity, or a presentation that requires professional assessment before continuing.
Nerve Flossing as Part of a Complete Neural Health Programme
Neural mobilisation is most effective when combined with postural management (addressing the positions that create sustained neural tension), targeted strengthening of the muscles whose weakness creates compressive loads on nerves, and activity modification during the acute phase. For sciatic nerve presentations, this means addressing hip abductor weakness that overloads the piriformis (often the compressing structure), correcting sitting posture that sustains lumbar flexion (increasing disc-related nerve compression), and gradually reintroducing the loaded activities that normal neural mobility should accommodate without symptoms.
Frequently Asked Questions About Nerve Flossing
How is nerve flossing different from just stretching the hamstrings for sciatica?
Hamstring stretching and sciatic nerve flossing both involve hip flexion with knee extension, but they target different structures and use different techniques. Hamstring stretching aims to lengthen the hamstring muscle-tendon unit by reaching and holding the end of available range. The sciatic nerve passes along the same anatomical pathway and is tensioned by the same movement, but the intent and technique are different: nerve flossing creates a rhythmic gliding motion of the nerve rather than a sustained tissue stretch.
The clinical difference matters: if hamstring stretching consistently aggravates rather than relieves sciatica symptoms, it is likely tensioning an already sensitised nerve beyond its tolerance rather than releasing tight muscle. Switching to the slider technique, which reduces sustained neural tension by alternating joint positions, typically produces the improvement that sustained hamstring stretching cannot provide in neural presentations. Many cases diagnosed as hamstring tightness in the context of posterior thigh and lower back pain are actually neural tension presentations that respond to nerve flossing rather than muscle stretching.
Is it safe to do nerve flossing every day?
Yes, daily nerve flossing with appropriate slider technique is safe and is the evidence-supported dosage for active neural tension presentations. The technique does not damage neural tissue when performed within pain-free range. The guideline that distinguishes appropriate from excessive dosage is the 30-minute response rule: symptoms should not be worse 30 minutes after completing a session than they were before the session. If they consistently are, reduce the range or frequency.
Tensioner techniques require more conservative application: every other day or three times per week rather than daily for most presentations, because the sustained neural tension they create requires more recovery time than the gentle slider gliding technique.
Why does my sciatica feel worse in the morning?
Morning worsening of sciatic symptoms reflects the overnight accumulation of neural oedema (fluid within the neural sheath) that accumulates during the sustained position of sleep and the reduction in lymphatic drainage that occurs with inactivity. The neural tissue becomes more sensitised overnight, producing greater symptoms with the first movements of the day. This pattern is a useful indicator of neural involvement rather than muscular tightness, which does not specifically worsen with the morning transition from rest to activity.
Performing a brief sciatic slider protocol immediately after waking, before loading activities, addresses the morning oedema peak and typically reduces the first-movement-of-the-day symptom severity. The pumping action of the slider technique disperses the accumulated neural oedema, reducing the neural sensitivity before the day’s activities begin.
Can nerve flossing help with plantar fasciitis?
A subset of plantar fasciitis presentations involves neural tension in the tibial nerve or its calcaneal branches alongside the plantar fascial irritation. In these mixed presentations, nerve flossing that mobilises the tibial nerve through the tarsal tunnel at the ankle, combined with standard plantar fascial loading exercises, produces better outcomes than plantar fascia treatment alone. The neural component is suspected when plantar heel pain is accompanied by tingling or burning rather than the pure mechanical ache of non-neural plantar fasciitis, and when symptoms extend toward the arch or toes in a pattern consistent with tibial nerve distribution.
How long does it take to see results from nerve flossing?
Acute presentations with primary neural oedema and sensitisation typically show measurable improvement within 3 to 7 days of twice-daily slider technique. Chronic presentations with structural adhesions, persistent compression from disc herniation, or significant central sensitisation require 4 to 8 weeks of consistent daily work before meaningful functional improvement occurs. The improvement timeline reflects the different mechanisms being addressed: acute inflammation and oedema respond quickly to the fluid dynamics of neural gliding, while structural adhesion release and central desensitisation require sustained repetitive loading over weeks.
- Neural mobilisation produces clinically meaningful reductions in pain and disability in lumbar radiculopathy across multiple RCTs. The evidence supports it as an effective non-surgical intervention for sciatica and radicular lower limb pain.
- Sliders create neural gliding with low peak tension and are appropriate for acute, irritated presentations. Tensioners create sustained neural tension and are appropriate for chronic, less sensitive presentations where tension tolerance is the goal.
- Begin with the supine sciatic slider for acute sciatica: 10 to 15 repetitions, twice daily, within pain-free range. Progress to seated and standing slider before introducing tensioner techniques.
- The 30-minute response rule determines technique appropriateness: symptoms that worsen during or after a session and do not return to baseline within 30 minutes indicate incorrect technique, excessive range, or a presentation requiring professional assessment.
- Neural mobilisation addresses nerve mobility and sensitivity. The underlying muscle imbalances, postural habits, and compressive structures that cause the neural tension also require attention for durable rather than temporary improvement.











