⚠️ Cardiovascular Monitoring Safety Note HRV monitoring is a wellness and performance tool — not a medical diagnostic device. Consistently low HRV accompanied by symptoms such as chest pain, unexplained breathlessness, palpitations, or severe fatigue may indicate an underlying cardiovascular or systemic condition requiring medical evaluation. Do not use HRV data alone to override symptoms that warrant professional assessment. Individuals with known arrhythmias or cardiac conditions should consult their physician before interpreting HRV data for training decisions.
Every athlete has experienced the day when the planned hard session feels wrong from the first warm-up rep — legs heavy, breathing laboured, intensity that should feel moderate hitting like near-maximum effort.
Heart rate variability (HRV) monitoring, done correctly, predicts that day the morning before training begins. It reads the nervous system’s readiness signal — the beat-to-beat variation in the heart that reflects the balance between sympathetic and parasympathetic activity — and tells you whether today’s biology supports the planned session or requires modification.
This guide explains what HRV actually measures, what the research shows about using it for training decisions, how to measure it reliably, and how to build a practical HRV-guided training system.
Research 1: What HRV Actually Measures and Why It Predicts Recovery
The Autonomic Nervous System Signal
The heart does not beat with metronome precision. Even at rest, the interval between consecutive heartbeats varies by tens to hundreds of milliseconds — a phenomenon called heart rate variability.
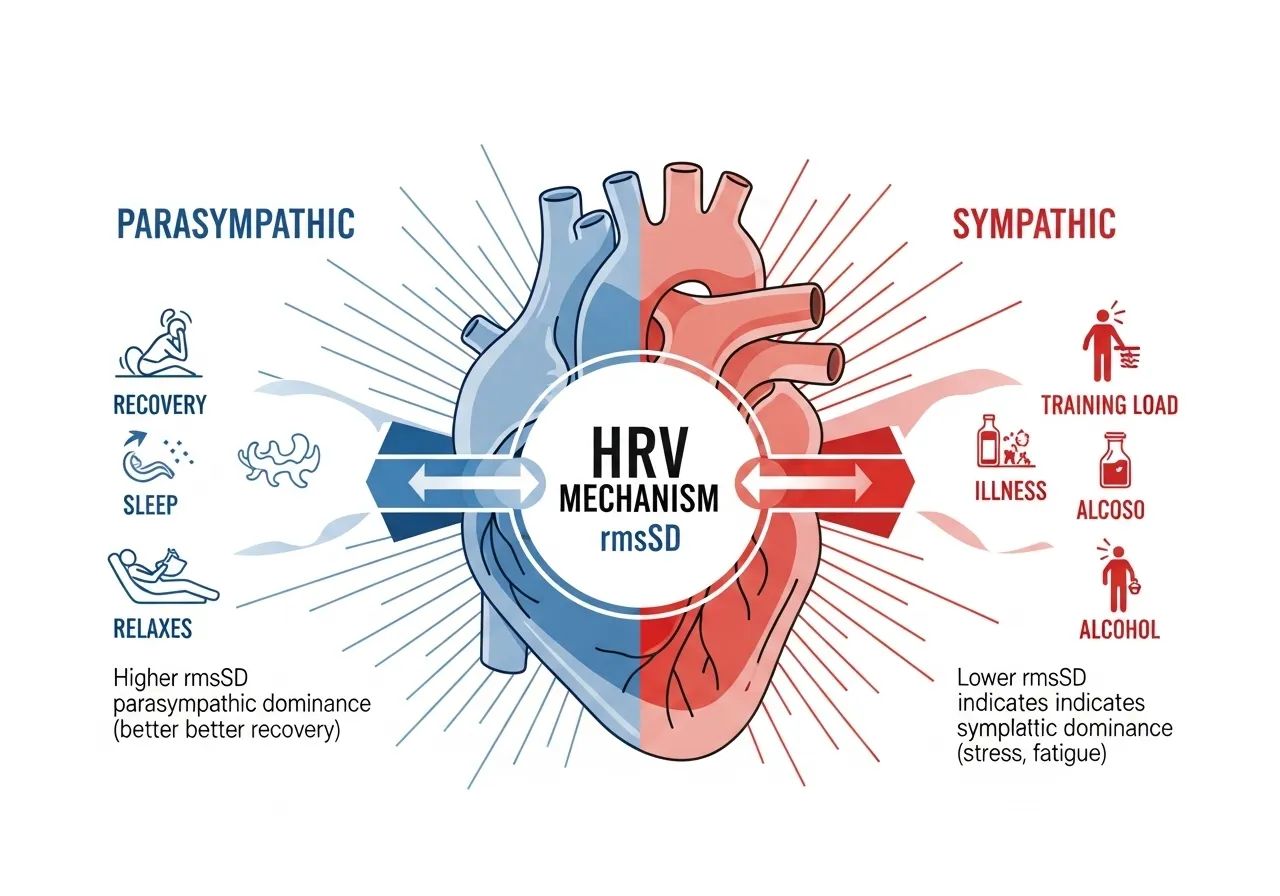
This variability reflects the ongoing competition between the sympathetic nervous system (fight-or-flight, stress response) and the parasympathetic nervous system (rest-and-digest, recovery). High HRV indicates strong parasympathetic influence — the body is recovered, well-rested, and ready for physiological stress. Low HRV indicates sympathetic dominance — the body is under stress, fatigued, or inadequately recovered.
The key metric in most consumer HRV applications is rmsSD (root mean square of successive differences) — a statistical measure of beat-to-beat variation that specifically reflects parasympathetic cardiac control. Higher rmsSD = greater parasympathetic activity = better recovery state.
📌 Key Finding
HRV-guided training reduces non-functional overreaching risk by quantifying recovery state before each session. The data allows training load adjustment on days when the nervous system signals incomplete recovery — preventing the accumulated fatigue that leads to overtraining.
What Depresses HRV: The Practical Signal List
Understanding what lowers HRV — beyond training load — is essential for interpreting daily readings correctly:
Training: Hard sessions (Zone 4–5) suppress HRV for 24–72 hours as the sympathetic nervous system processes the training stress
Alcohol: Even moderate alcohol consumption suppresses HRV the following morning — the most sensitive and consistent HRV response to a lifestyle variable
Poor sleep: Both sleep quantity below 7 hours and poor sleep quality reduce morning HRV measurably
Illness: HRV drops before symptoms appear — an early warning system that is often detectable 12–24 hours before the trainee feels unwell
Psychological stress: Emotional and cognitive stress elevates sympathetic activity and reduces HRV independently of physical training load
Heat and dehydration: Both shift autonomic balance toward sympathetic dominance and reduce rmsSD readings
Research 2: HRV-Guided Training Outperforms Fixed Training Schedules
📌 Key Finding
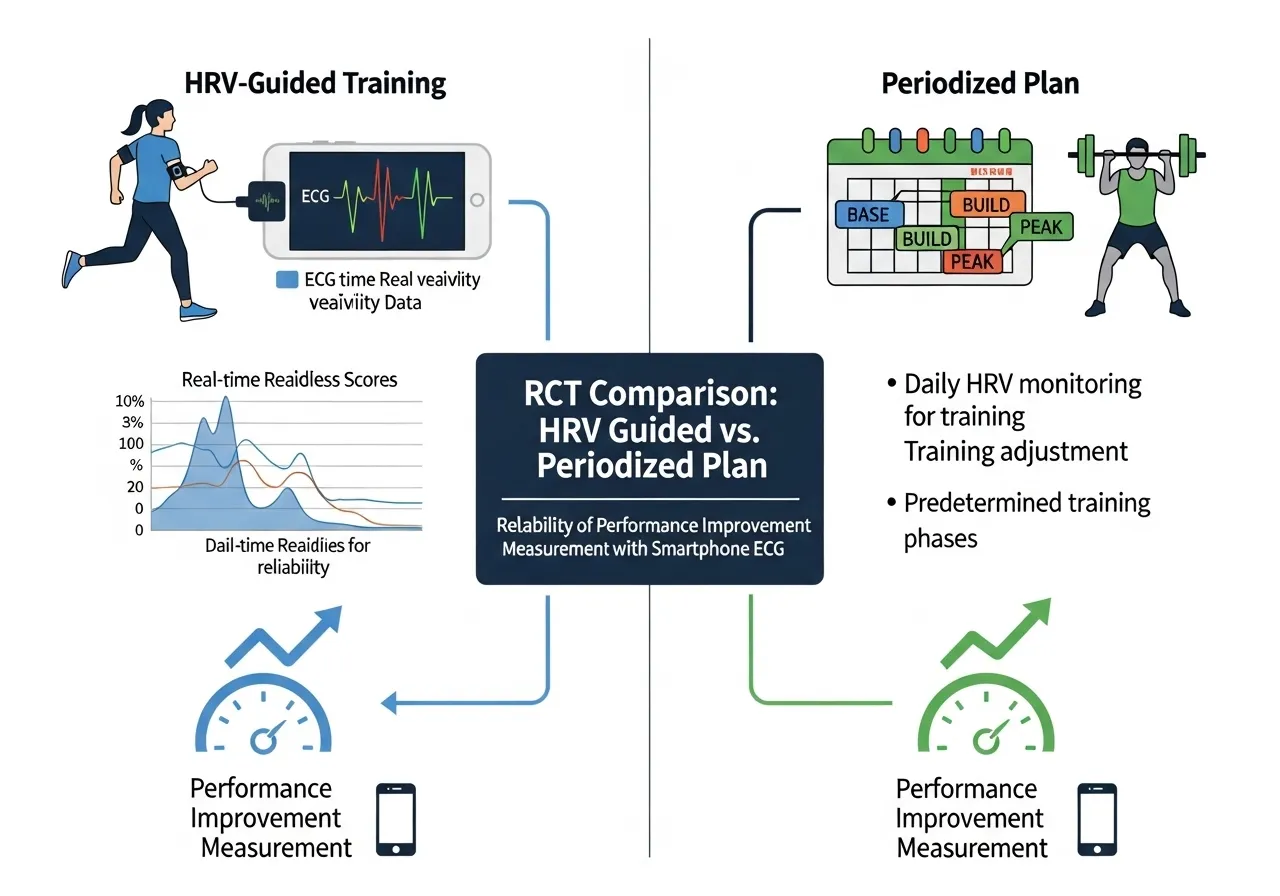
HRV-guided athletes trained more on high-HRV days and less on low-HRV days — producing greater total adaptation than fixed plans, despite similar average weekly load. The flexibility to capitalise on good recovery days is as important as protecting bad ones.
📌 Key Finding
Smartphone HRV apps with chest straps or pulse sensors produce reliable data comparable to ECG when measured correctly — making HRV monitoring accessible without expensive medical equipment.
What the Research Does Not Support
HRV research has clear boundaries worth understanding:
Single readings are not meaningful: A single low HRV morning means almost nothing. The signal that matters is deviation from your personal 7–14 day rolling baseline — not the absolute number compared to published norms
HRV does not predict injury: Research on HRV as a direct injury predictor shows inconsistent results. It predicts recovery and readiness state; injury risk inference is speculative
HRV cannot replace subjective readiness: Perceived readiness, motivation, and qualitative sleep quality each provide information that HRV does not capture. The data complements — not replaces — self-awareness
Is HRV Monitoring Worth the Effort — or Just Another Metric to Obsess Over?
The Valid Concern
HRV monitoring attracts legitimate criticism: it adds complexity to training, the numbers can create anxiety, and the temptation to skip planned sessions whenever HRV looks suboptimal can reduce overall training volume below what produces adaptation.
These concerns are real. Poorly implemented HRV monitoring — checking the number obsessively, changing every session based on small fluctuations, treating low HRV as a prohibition rather than a signal — often produces worse training outcomes than ignoring it entirely.
The Evidence-Based Use Case
HRV monitoring produces the greatest benefit in two specific contexts:
High-training-load athletes: Athletes training 8–15+ hours per week who regularly push close to their recovery limits benefit most from objective recovery monitoring. The margin between adequate loading and overreaching is narrow; HRV provides the early warning system that prevents crossing it unknowingly.
Return from illness or travel: HRV reliably tracks the recovery of autonomic function after illness, sleep disruption from time zone changes, and accumulated life stress. The data confirms when the body has genuinely recovered versus when it merely feels recovered — preventing premature return to hard training.
The Diminishing Returns for Recreational Athletes
For recreational athletes training 3–5 hours per week at moderate intensities, the marginal benefit of HRV monitoring is lower. At this training volume, the consequences of training on a sub-optimal day are modest, and the recovery windows between sessions are long enough that monitoring adds limited decision value.
The honest recommendation: HRV monitoring is most valuable for athletes training 6+ hours per week or in competitive preparation phases. For general fitness trainees, the subjective measures of sleep quality, energy levels, and motivation provide comparable guidance with less complexity. See also: Zone 2 training guide for how HRV integrates with a heart rate zone training framework.
HRV and Sleep: The Most Actionable Relationship
Of all the variables that influence HRV, sleep quality and quantity produce the most consistent and largest effects. A single night of 5-hour sleep depresses HRV measurably the next morning; chronic mild sleep restriction (6 hours per night for a week) progressively reduces baseline HRV without any change in training load.
For most recreational athletes, sleep optimisation produces larger HRV improvements — and therefore larger training adaptation gains — than any change to the training programme itself. If morning HRV is chronically lower than expected, the first variable to address is sleep quality and duration before adjusting training load or adding recovery protocols. The data makes this priority ordering objective rather than speculative.
HRV During Illness: The Most Reliable Early Warning
HRV reliably drops before subjective illness symptoms appear — often by 12–24 hours. Athletes who train through a low-HRV period that turns out to be early illness consistently report that the session felt far harder than expected and extended their recovery timeline significantly.
When HRV drops unexpectedly below the red threshold with no corresponding training load explanation, illness is a likely cause. The correct response: reduce to easy training only, prioritise sleep, and monitor the trend. Most viral illnesses produce 3–5 days of suppressed HRV before baseline recovery begins. Training hard during this window prolongs the suppression and delays full recovery.
How to Measure HRV Correctly: Protocol, Tools, and Common Errors
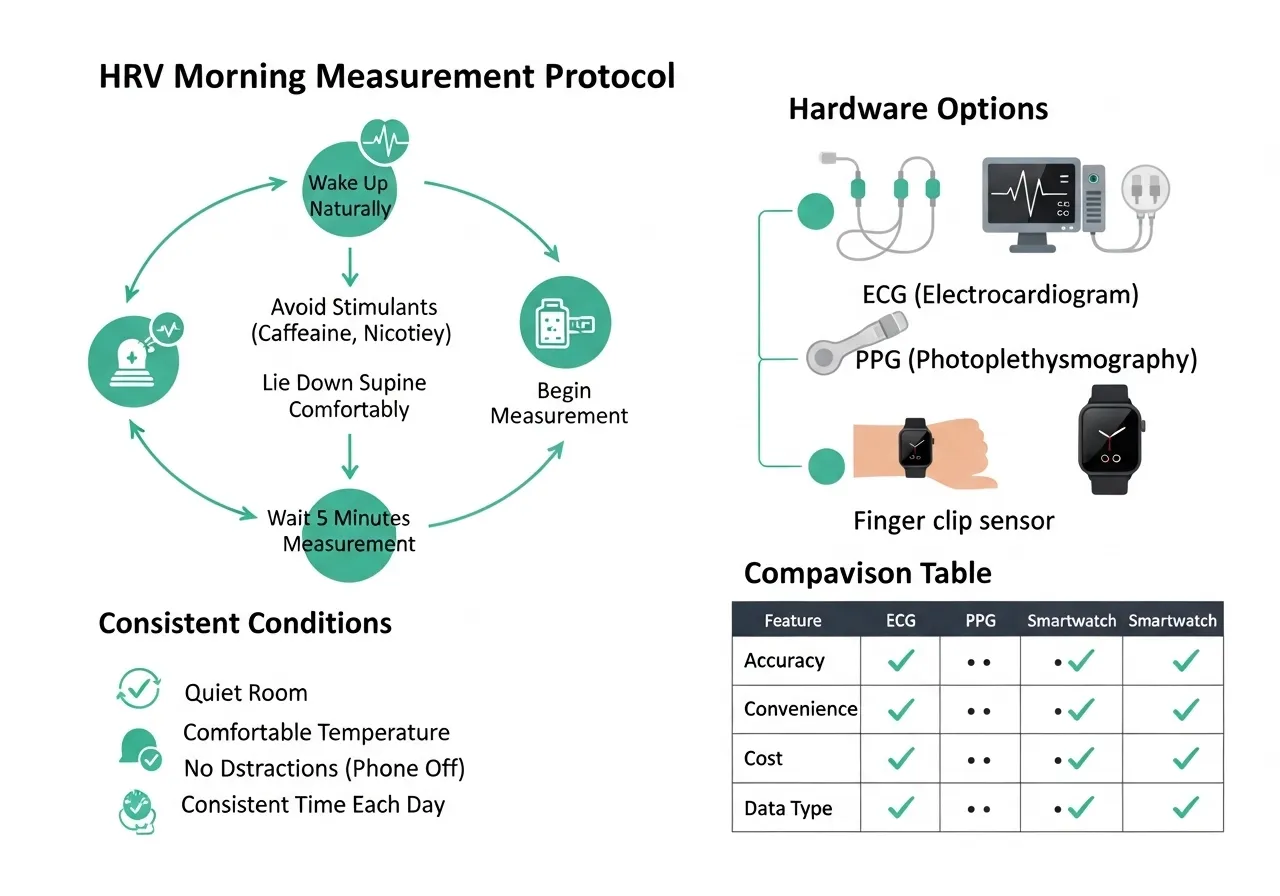
The Measurement Protocol That Produces Reliable Data
HRV measurement is protocol-sensitive — small deviations in measurement conditions produce significant day-to-day variability that overwhelms the genuine biological signal. The standardised protocol:
Timing: Immediately upon waking, before getting out of bed, before coffee or food
Position: Supine (lying on back) — not sitting or standing, which significantly reduce rmsSD readings
Duration: 3–5 minutes continuous measurement — not the 60-second ultra-short protocols that many apps use
Consistency: Same time, same position, same device, every day — the baseline is meaningless if the measurement conditions vary
Hardware Options
Device Type
Accuracy
Cost
Best For
ECG chest strap (Polar H10)
Gold standard
£70–100
Athletes requiring highest precision
PPG chest/wrist strap
High (validated)
£30–70
Most practical option for daily use
Smartwatch (Garmin, Whoop, Oura)
Moderate-High
£150–500+
Passive overnight measurement
Smartphone camera (PPG)
Moderate
Free (app only)
Beginners testing the concept
Interpreting Your Numbers
HRV values vary enormously between individuals — a rmsSD of 40ms may indicate excellent recovery for one person and poor recovery for another. The meaningful comparison is always your current reading versus your personal baseline, not your number versus published norms.
Most HRV apps automatically calculate a rolling 7–14 day baseline and display today’s reading as a percentage of that baseline — green (above baseline = high readiness), amber (near baseline = moderate readiness), red (below baseline = low readiness). This relative scoring is more actionable than the absolute millisecond value.
Establishing a reliable personal baseline requires 2–4 weeks of consistent daily measurement under identical conditions. Readings during this period should not influence training decisions — the baseline is being calibrated.
How to Use HRV Data to Make Better Training Decisions
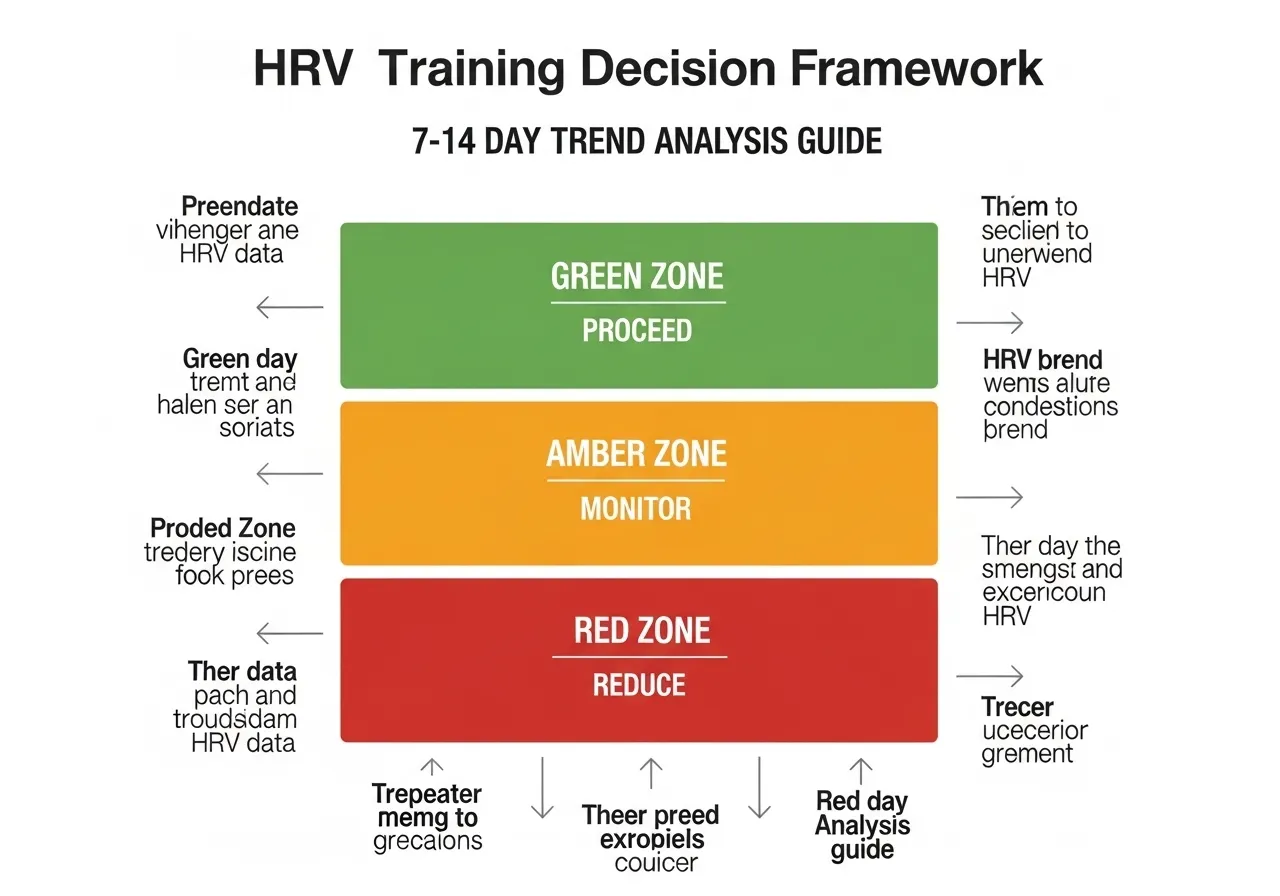
The Three-Zone Decision Framework
Rather than trying to interpret every HRV fluctuation, use a simple three-zone framework based on deviation from your rolling baseline:
HRV Status
Deviation from Baseline
Training Recommendation
🟢 High
+5% or more above baseline
Proceed as planned; consider adding intensity if feeling good
🟡 Normal
Within ±5% of baseline
Train as planned; monitor effort response during session
🔴 Low
More than 5% below baseline
Reduce intensity to Zone 2; postpone hard session by 24 hours
The HRV-Guided Training Week
A practical weekly structure that integrates HRV data without creating paralysis:
Scheduled hard days (Zone 4–5): Proceed if HRV is green or yellow. Postpone to the next day if red — rarely more than one day postponement is needed.
Scheduled easy days (Zone 1–2): Proceed regardless of HRV — easy sessions do not significantly stress the system and may actually improve HRV by promoting recovery.
Unscheduled green HRV days: The RCT data shows that performing additional quality work on high-HRV days produces the performance advantage of HRV guidance. If Monday’s planned easy run shows green HRV, consider upgrading it to a moderate tempo run.
Trend Analysis: The Signal That Matters Most
Daily HRV fluctuations are relatively noisy — influenced by minor variations in sleep position, evening food, and hydration. The more meaningful signal is the 7–14 day trend: is your baseline HRV rising (positive adaptation to training), stable (maintenance), or falling (accumulated fatigue or overreaching)?
A steadily declining baseline over 2–3 weeks despite normal training loads signals that recovery is not keeping pace with stress — and warrants a reduction in training load or additional rest days before the system reaches a symptomatic state. See also: HIIT training guide for how to structure high-intensity sessions around HRV data for optimal adaptation without overreaching.
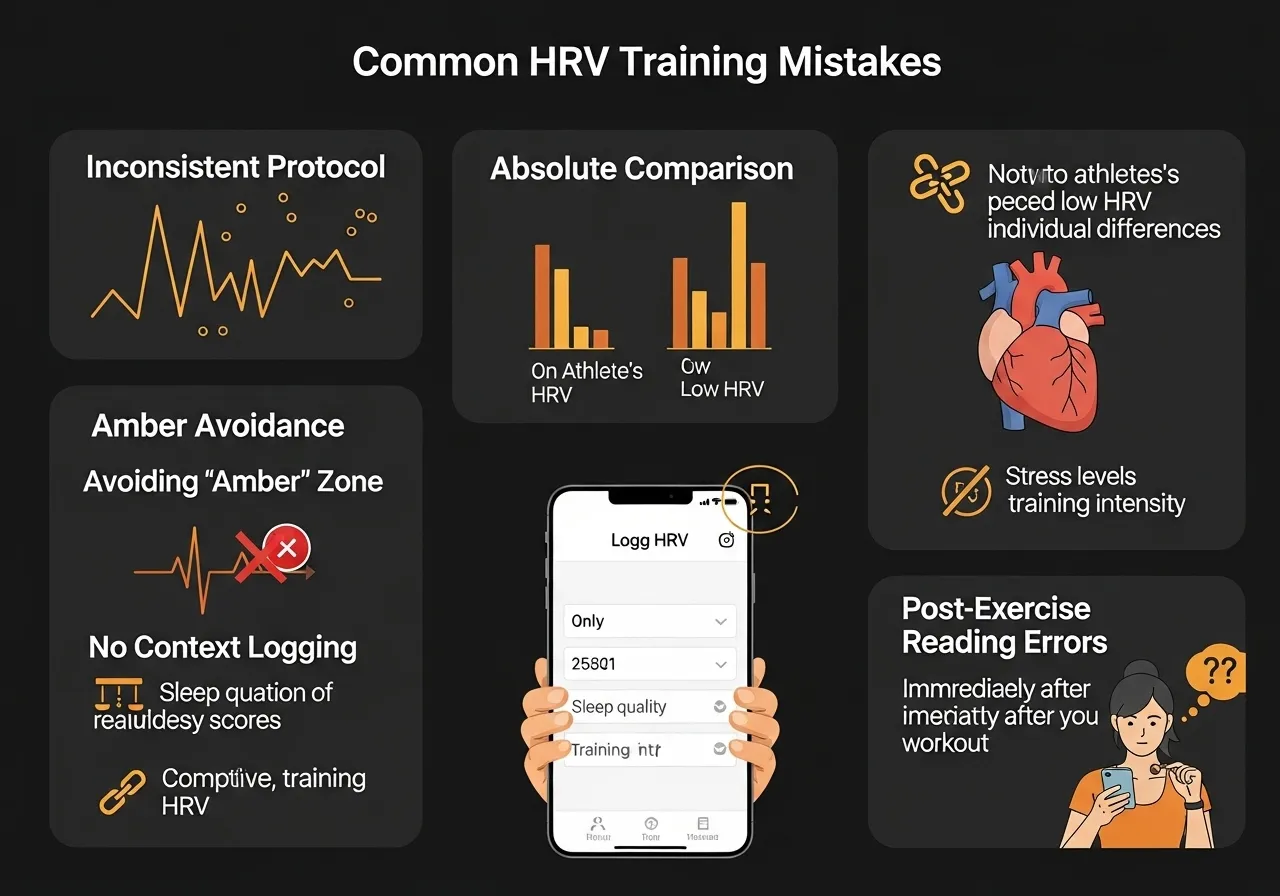
5 HRV Monitoring Mistakes That Produce Useless Data
Mistake 1: Inconsistent Measurement Conditions
Measuring some days supine and others sitting, some days at 6 AM and others at 9 AM, some days with a chest strap and others with a phone camera — creates a dataset where genuine biological variation is indistinguishable from measurement noise. The resulting numbers are not interpretable.
Establish one fixed protocol and never deviate from it. The investment in a chest strap or dedicated HRV device — used consistently — produces far more actionable data than an expensive smartwatch used inconsistently.
Mistake 2: Interpreting Absolute Numbers Without a Personal Baseline
A rmsSD of 35ms does not mean the same thing for every person. For one athlete, 35ms is their normal rested baseline; for another, it represents significant depression from a normal of 65ms. Comparing absolute numbers between individuals — or comparing your number to published “normal” ranges — produces misleading interpretations.
Always interpret relative to your own rolling baseline. The app’s colour-coded readiness score does this automatically — trust the relative score rather than the absolute number.
Mistake 3: Skipping Sessions Every Time HRV Is Amber
The amber (near-baseline) zone does not mean do not train. It means train as planned with awareness. Skipping every amber day reduces weekly training volume significantly without meaningful recovery benefit — amber is a signal to monitor the session quality, not a prohibition to train.
Mistake 4: Not Logging Context Alongside HRV
HRV data without contextual notes is difficult to interpret retrospectively. Logging sleep hours, alcohol (yes/no), perceived stress, and travel alongside daily HRV readings allows pattern recognition — identifying which lifestyle variables most predictably suppress your personal HRV, and quantifying the magnitude of their effect. This retrospective analysis is where HRV monitoring becomes genuinely individualised rather than generic.
Mistake 5: Measuring During or Immediately After Training
HRV measured during or within 30 minutes of training or intense activity reflects the acute cardiovascular response to exercise — not resting autonomic state. Post-exercise measurements are physiologically meaningless for recovery monitoring. The valid measurement window is morning, before getting up, after 5+ hours of sleep.
The Over-Reliance Problem: When HRV Becomes a Crutch
A subtle but important risk in HRV monitoring: developing excessive dependence on the number to the point where training decisions become paralysed by the data rather than informed by it.
HRV provides one signal about one physiological system. Experienced athletes develop intuition about their readiness through years of training — an intuition that integrates far more information than a single morning measurement. HRV should add precision to this intuition, not replace it. If the number says green but the body clearly signals fatigue, trust the body. If the number says red but everything feels genuinely good, proceed cautiously with awareness rather than cancelling automatically. The data informs decisions; it does not make them.
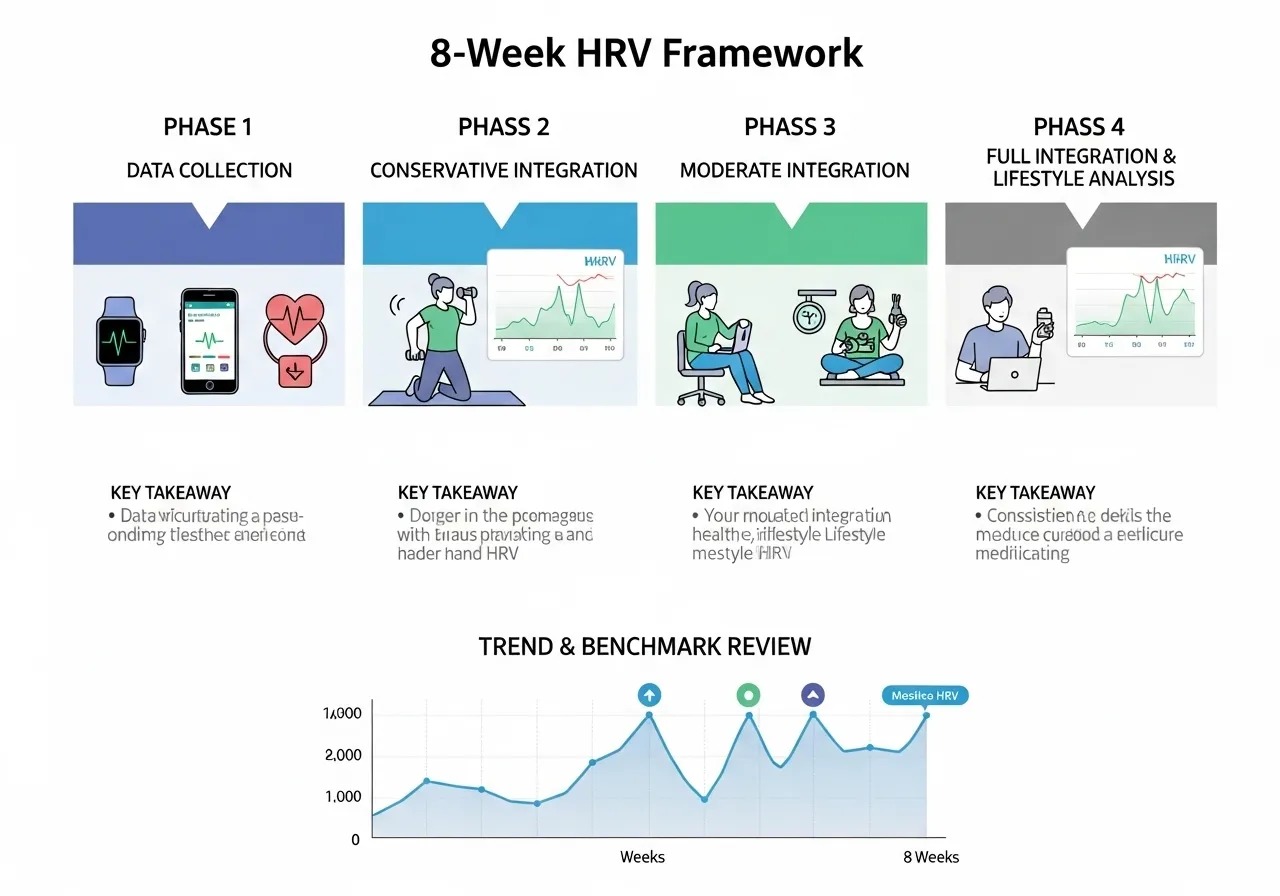
8-Week HRV-Guided Training Framework
This framework does not prescribe specific workouts — it provides the decision structure for integrating HRV data into any existing training programme. The 8 weeks follow a progressive structure from baseline establishment through full HRV integration.
Equipment: any validated HRV measurement device or app. Recommended: Polar H10 chest strap + HRV4Training app, or equivalent.
Review 7-day rolling baseline trend — is it rising, stable, or falling?
If declining trend without increased training load: identify and address recovery limiter (sleep, stress, nutrition)
8-week benchmark: Compare Week 7–8 average HRV baseline to Week 1–2 baseline. A rising baseline indicates positive adaptation to training. Has your training decision quality improved? Have you avoided the overreaching episodes that a fixed schedule might have produced?
Focus: The 8-week review assesses whether HRV monitoring improves training quality and recovery — if the correlation between HRV and performance is weak for you personally, the approach may not justify the monitoring overhead
Frequently Asked Questions About Heart Rate Variability
What is a good HRV number?
There is no universal “good” HRV number. Values range from below 20ms rmsSD in sedentary older adults to above 100ms in elite endurance athletes — with enormous individual variation. The relevant question is not “is my number good?” but “is my number above or below my personal baseline today?” A trained athlete with a baseline of 45ms and a reading of 35ms has significantly suppressed HRV; a sedentary individual with a baseline of 25ms and a reading of 28ms shows above-average readiness — despite the trained athlete’s absolute number being higher.
Should I train when HRV is low?
Depends on the session type. Easy training (Zone 1–2) on a low-HRV day is generally appropriate — it does not add significant autonomic stress and may facilitate recovery. Hard training (Zone 4–5) on a significantly low-HRV day typically produces poor performance, inadequate adaptation, and contributes to the continued suppression of HRV. The practical guideline: reduce intensity to Zone 2 on red-HRV days; postpone planned hard sessions by 24 hours when possible.
Which HRV app should I use?
Elite HRV, HRV4Training, and Whoop are the most research-validated consumer HRV platforms. All three use established rmsSD calculation and provide reliable baseline tracking with contextual logging. The device matters as much as the app: a validated chest strap (Polar H10) with any of these apps produces more reliable data than a smartwatch alone for morning HRV measurement. For those committed to passive overnight monitoring without a morning protocol, Whoop and Oura Ring provide the most consistent overnight HRV tracking.
Does HRV improve with training?
Generally yes — endurance training progressively improves resting HRV through increased cardiac vagal tone (parasympathetic nervous system influence on the heart). Athletes typically show higher resting HRV than sedentary individuals, and sustained aerobic training produces upward baseline HRV trends over months. However, very high training loads without adequate recovery can produce a declining HRV trend despite fitness improvement — a pattern that distinguishes functional overreaching from non-functional overreaching.
Can HRV replace other recovery metrics?
No — HRV complements but does not replace subjective readiness, sleep quality assessment, perceived effort monitoring, and periodic performance testing. Each metric captures different aspects of readiness that the others miss. The most complete recovery monitoring uses HRV alongside sleep quality (hours + subjective quality), perceived readiness (1–10 scale), and periodic performance benchmarks to provide a multi-dimensional picture of adaptation. See also: VO2max guide for how HRV trends correlate with the aerobic fitness markers that HRV-guided training is designed to improve.
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only and does not replace professional medical or fitness advice.If you have any cardiovascular condition, joint concerns, or are new to vigorous exercise — consult a qualified healthcare professional before starting any HIIT program. High-intensity interval training — HIIT — has moved…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only and does not replace professional medical advice. If you have any lower back, knee, or cardiovascular conditions, please consult a qualified healthcare professional before beginning a rowing machine mastery guide program. The rowing machine training guide machine — or ergometer — produces a…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only. It does not replace professional medical advice. If you have cardiovascular, joint, or respiratory conditions, consult a qualified healthcare professional before beginning a running programme. Running is the most accessible cardiovascular exercise on the planet. No equipment, no membership, no learning curve —…
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only. It does not replace professional medical or fitness advice. If you have any pre-existing condition, injury, or health concern — consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program. VO2 max is one of…
Three minutes of actual sprint work per week produces the same VO2 max improvement as five full hours of moderate-intensity cycling per week. This is not a headline designed to sell something. It is the finding of a peer-reviewed randomised controlled trial from McMaster University. Sprint interval training operates through a different physiological mechanism than…
⚠️ Health & Fitness DisclaimerThis article is for general educational and informational purposes only.It does not replace professional medical or fitness advice.If you have any pre-existing condition, injury, or cardiovascular concern — please consult a qualified healthcare professional or certified personal trainer before starting or modifying any exercise program. Battle ropes sit at an unusual…


")








