
Shoulder Internal Rotation: Why GIRD Affects Athletes and Desk Workers Equally and How to Restore the Range
Shoulder internal rotation is one of the most commonly restricted ranges of motion in both overhead athletes and office workers, for completely different reasons that produce the same mechanical consequence: the humeral head cannot sit centrally in the glenoid during overhead movements, the supraspinatus tendon gets compressed, and pain or injury follows.
In overhead athletes — pitchers, swimmers, volleyball players — the restriction develops because the posterior capsule and posterior rotator cuff thicken in response to the eccentric deceleration demands of throwing and swinging. In desk workers, the restriction develops because the sustained forward-head, rounded-shoulder posture shortens the anterior shoulder structures and neurologically inhibits the posterior external rotators, creating a different pattern of internal rotation restriction from the athlete but one that produces similar mechanical consequences during the overhead movements of daily life.
This guide covers the anatomy of shoulder internal rotation restriction, what the research shows about the sleeper stretch and cross-body stretch for restoring glenohumeral internal rotation deficit, how to differentiate capsular restriction from muscular tightness, specific protocols for athletes and desk workers, and the thoracic spine connection that many shoulder internal rotation programmes miss.
The Anatomy and Mechanics of Shoulder Internal Rotation Restriction
Glenohumeral Internal Rotation: What the Motion Actually Involves
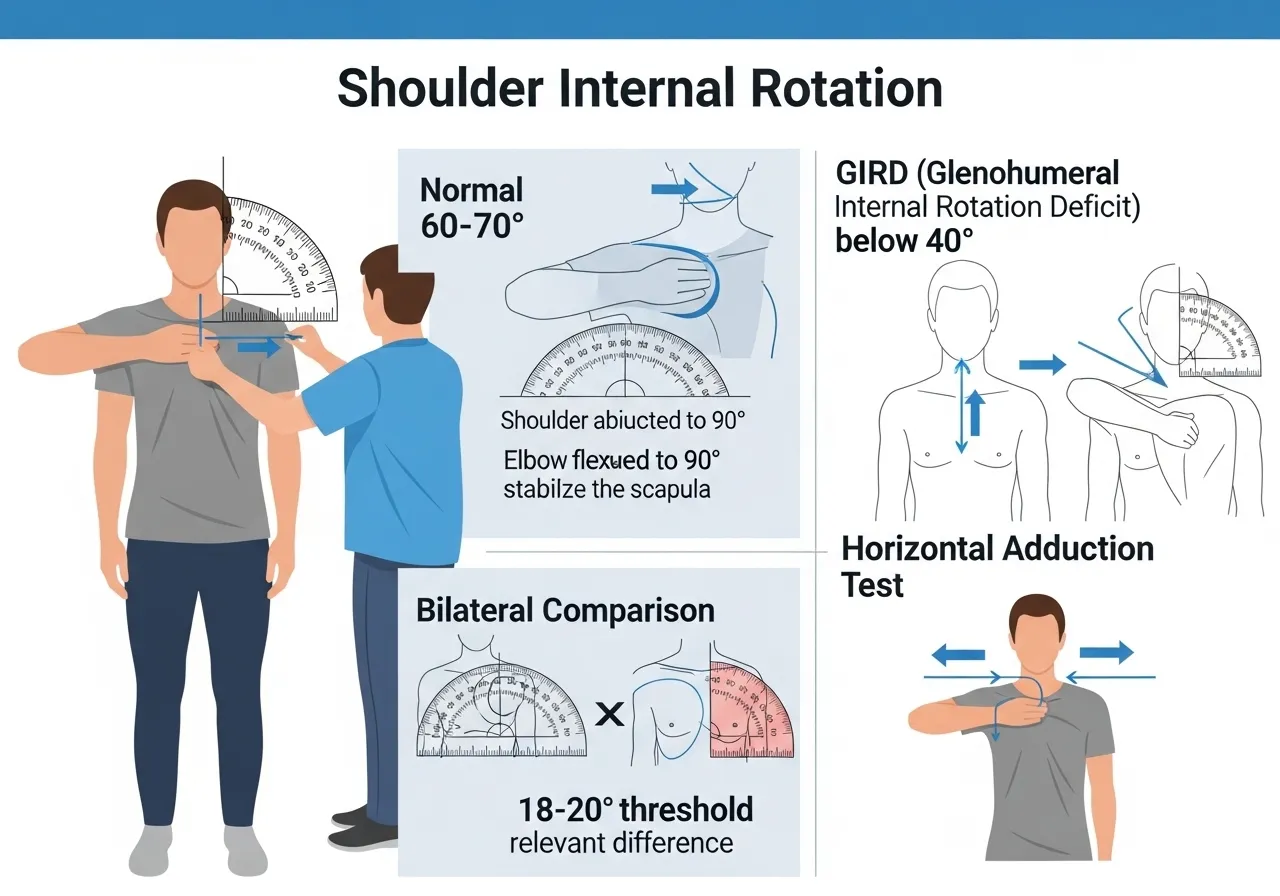
Glenohumeral internal rotation is the rotation of the humerus within the glenoid fossa of the scapula, measured with the shoulder at 90 degrees of abduction and the elbow flexed to 90 degrees. Normal glenohumeral internal rotation range is approximately 60 to 70 degrees, though this varies significantly between individuals and between dominant and non-dominant shoulders in athletes. When this range falls below 25 degrees at 90 degrees of abduction, the clinical definition of glenohumeral internal rotation deficit (GIRD) is met for most clinical assessment systems.
The motion requires the posterior capsule of the glenohumeral joint, the posterior rotator cuff (infraspinatus and teres minor), and the posterior glenohumeral ligaments to lengthen and allow the humeral head to rotate internally within the socket. When any of these structures are tight, shortened, or thickened, internal rotation range is limited — and the mechanical consequence is that the humeral head cannot maintain its centred position during overhead movement.
The Posterior Capsule: The Primary Restricting Structure
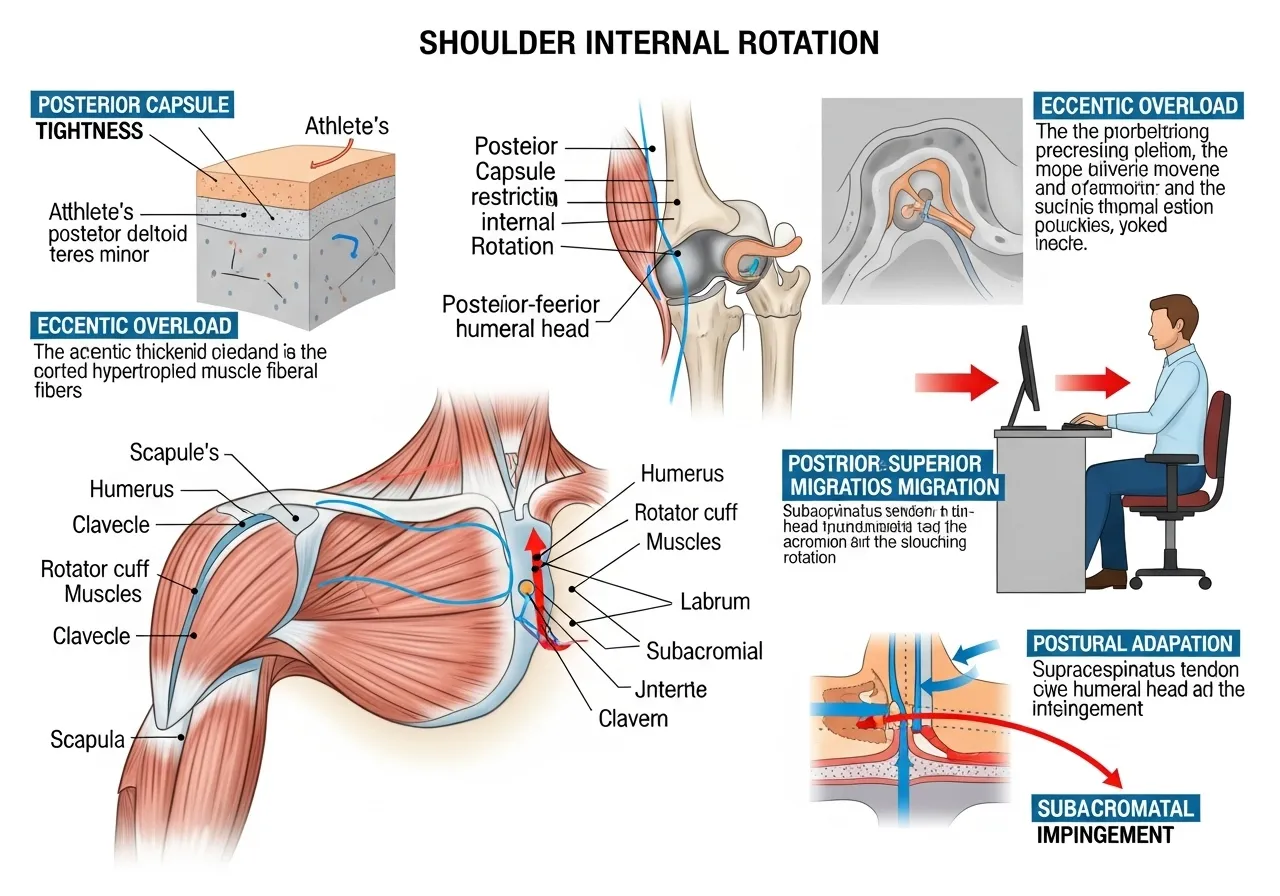
The posterior glenohumeral capsule is the most commonly identified structural cause of internal rotation restriction in both athletes and non-athletes. In overhead athletes, the posterior capsule thickens through adaptive hypertrophy in response to the repetitive eccentric loading of the external rotators during the arm deceleration phase of throwing. This adaptive thickening is an appropriate structural response to high eccentric loads, but it progressively restricts internal rotation as the capsule’s stiffness increases beyond the range needed for normal glenohumeral mechanics.
In non-athletes, the posterior capsule tightens through postural habituation. Sustained positions of shoulder internal rotation and protraction, characteristic of desk work and screen use, create persistent low-grade posterior capsule compression that gradually reduces posterior capsule extensibility. The mechanism differs from the athlete’s eccentric loading adaptation, but the structural consequence — a stiffer posterior capsule that restricts internal rotation — is similar in its effects on overhead mechanics.
GIRD and Supraspinatus Impingement: The Injury Mechanism
When the posterior capsule restricts internal rotation, the humeral head is pushed anteriorly and superiorly within the glenoid during overhead motion rather than remaining centred. This abnormal humeral head migration compresses the supraspinatus tendon and the subacromial bursa between the humeral head and the undersurface of the acromion during shoulder elevation. The result is the subcoracoid or subacromial impingement pattern that produces anterior shoulder pain with overhead movements — the most common shoulder pain complaint in both athletes and office workers performing overhead tasks.
External Rotation Gain: The Adaptive Compensation
Athletes with GIRD typically develop a compensatory increase in glenohumeral external rotation range on the dominant side that partially offsets the internal rotation loss. The total arc of rotation (internal rotation plus external rotation) may be maintained approximately constant even as internal rotation decreases and external rotation increases. This compensation maintains throwing mechanics but creates asymmetric rotator cuff loading that is associated with higher risk of SLAP (superior labral anterior to posterior) tears and posterior rotator cuff pathology in high-volume throwing athletes.
How Desk Worker GIRD Differs From Athlete GIRD
Desk worker GIRD typically involves both glenohumeral restriction and thoracic restriction simultaneously. The rounded thoracic posture of prolonged sitting reduces thoracic extension mobility, which forces the scapula into downward rotation and protraction, which reduces the effective range of shoulder elevation before impingement occurs. Addressing desk worker GIRD requires both posterior glenohumeral capsule restoration through targeted stretching and thoracic extension restoration through mobility work. The thoracic rotation and extension mobility that underpins normal shoulder mechanics is covered in the thoracic rotation guide.
Research: Sleeper Stretch vs Cross-Body Stretch for GIRD Restoration
The Two Standard GIRD Interventions
Two stretching techniques dominate the clinical and research literature on GIRD management: the sleeper stretch and the cross-body (or horizontal adduction) stretch. Both target the posterior glenohumeral capsule and posterior rotator cuff but through different joint positions and force vectors. The sleeper stretch positions the shoulder in 90 degrees of abduction in the side-lying position and applies an internal rotation force. The cross-body stretch positions the shoulder in horizontal adduction, stretching the posterior capsule through a different angle that many practitioners find more comfortable and controllable than the sleeper stretch.
Novel Stretch vs Modified Sleeper Stretch: RCT Evidence
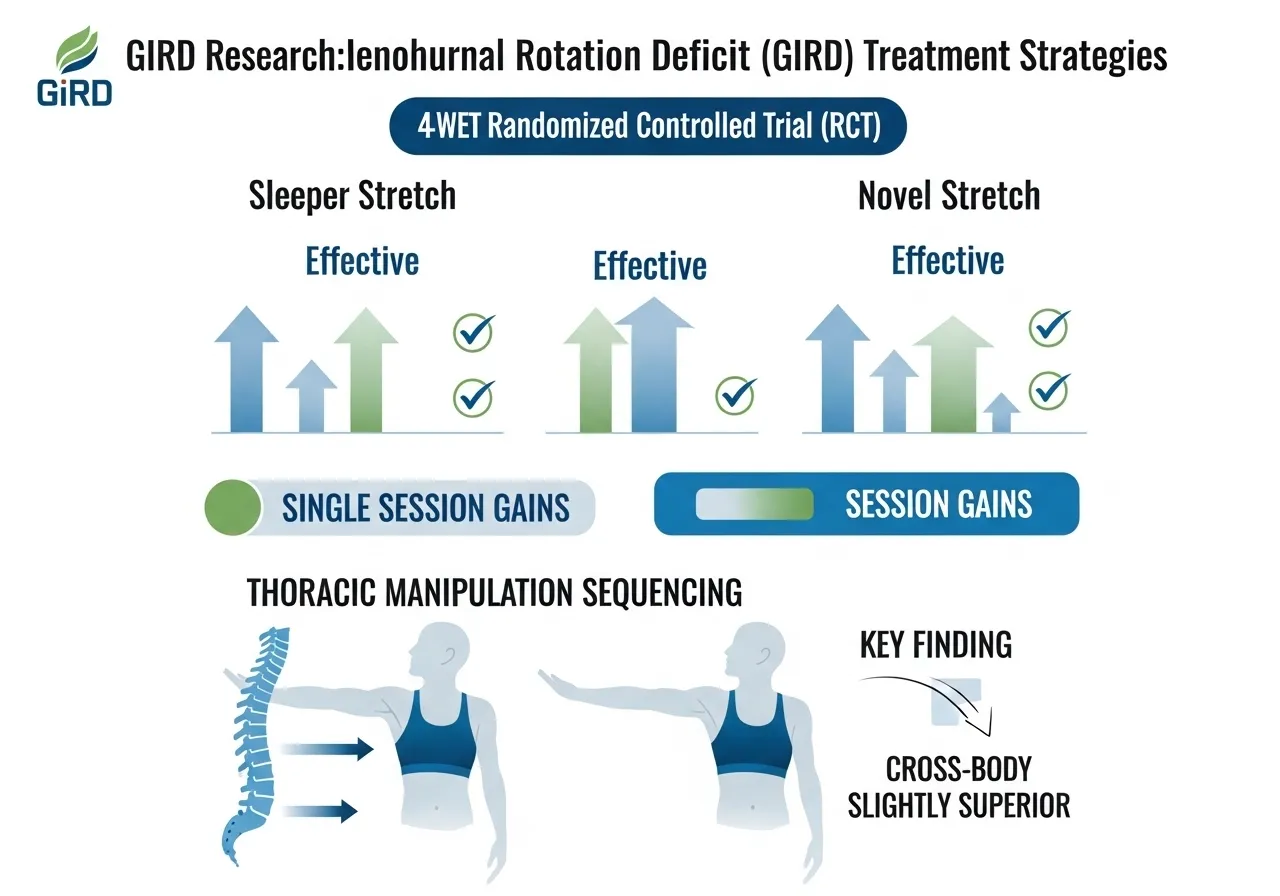
A randomised controlled trial examining the effect of a novel stretching technique on shoulder range of motion in overhead athletes with glenohumeral internal rotation deficits found that there was no significant group by time interaction effect for internal rotation range of motion between novel and modified sleeper stretch groups, however there was a significant change over time with both groups showing meaningful improvements in glenohumeral internal rotation range of motion, with the study confirming that consistent application of posterior capsule stretching techniques over a 4-week period produces clinically significant improvements in shoulder internal rotation range of motion regardless of which specific technique is used, suggesting that patient tolerance and comfort may be reasonable criteria for technique selection between sleeper and alternative posterior capsule stretches.
Both sleeper stretch and novel alternatives produce significant internal rotation ROM improvements over 4 weeks. Consistent application matters more than which specific posterior capsule technique is used — patient comfort and tolerance are valid selection criteria between techniques.
Glenohumeral Mobilisation and Sleeper Stretch Combined With Thoracic Manipulation
A study examining the combined effects of glenohumeral mobilisation, stretching, and thoracic manipulation on shoulder internal rotation range of motion found that both glenohumeral posterior mobilizations and sleeper stretches improved internal rotation and horizontal adduction passive range of motion in a single session, and that the addition of thoracic manipulation prior to local shoulder interventions resulted in smaller gains of both internal rotation and horizontal adduction range of motion than local shoulder interventions alone, confirming that glenohumeral posterior mobilizations and sleeper stretches are effective standalone interventions for immediate internal rotation gains and that local shoulder interventions should precede rather than follow thoracic manipulation in treatment sequencing.
Glenohumeral mobilisation and sleeper stretches produce immediate internal rotation gains within a single session. Local shoulder interventions should precede thoracic manipulation in treatment sequencing — contrary to the intuitive approach of addressing thoracic mobility first.
Sleeper Stretch vs Cross-Body Stretch: Which Is Superior?
Research comparing the sleeper stretch directly to the cross-body stretch for GIRD management finds both techniques produce significant internal rotation improvements with consistent application, and that the cross-body stretch tends to produce slightly greater improvements in some studies. A study comparing these two techniques found that both sleeper and cross-body stretches improved internal rotation range of motion in overhead athletes with GIRD, and that the cross-body stretch was slightly superior to the sleeper stretch in most outcome measures but that the study was underpowered to show a statistically significant difference between the two interventions, with the practical conclusion being that both techniques are effective and that patient preference and comfort are appropriate selection criteria when both are available.
Both sleeper and cross-body stretches improve GIRD with consistent application. Cross-body stretch may be slightly more effective, but the difference is small enough that patient comfort and preference are practical selection criteria.
How Long Does GIRD Restoration Take?
Research on GIRD restoration timelines consistently shows measurable improvements within 4 to 8 weeks of daily posterior capsule stretching. Acute gains of 5 to 15 degrees of internal rotation are achievable in a single session with immediate posterior capsule mobilisation or stretching, confirming that the restriction is predominantly viscoelastic (stretch-responsive) rather than structural. Sustained restoration requiring 4 to 8 weeks of daily work reflects the time required for the posterior capsule’s structural adaptation to the repeated stretch stimulus rather than the time for a single viscoelastic response.
How Do You Know If You Have a Shoulder Internal Rotation Deficit Worth Treating?
The Clinical Assessment Method
The standard clinical assessment for glenohumeral internal rotation measures passive internal rotation with the shoulder at 90 degrees of abduction and the elbow at 90 degrees of flexion. Lie on the back with the testing arm abducted to 90 degrees and the elbow bent to 90 degrees, forearm pointing toward the ceiling. A partner stabilises the scapula against the table by pressing gently on the anterior shoulder to prevent scapular compensatory rotation. The arm is then internally rotated (forearm moves toward the table on the same side as the arm) until the end of passive range or the scapula begins to move.
Normal range is approximately 60 to 70 degrees from the neutral forearm-pointing-to-ceiling position. A range below 40 degrees indicates significant restriction. Comparing both sides provides more clinically useful information than an absolute measurement: a side-to-side difference greater than 18 to 20 degrees is the most commonly cited clinical threshold for GIRD in athletes.
Differentiating Posterior Capsule Restriction From Rotator Cuff Tightness
The sleeper stretch position can help differentiate between posterior capsule restriction and posterior rotator cuff (infraspinatus/teres minor) tightness as the primary restriction. During the sleeper stretch, if the stretch sensation is felt deep within the shoulder joint rather than in the posterior rotator cuff muscle belly, the capsule is the primary restrictor. If the stretch is felt primarily in the posterior rotator cuff musculature outside the joint, the soft tissue is the primary restrictor. This distinction matters for intervention selection: capsular restriction responds better to sustained low-load stretching and joint mobilisation; muscular restriction responds better to active and dynamic stretching techniques.
The Scapular Compensation Test
One of the most common assessment errors in shoulder internal rotation measurement is allowing the scapula to compensate by rotating anteriorly as the arm internally rotates, giving a falsely high internal rotation reading because the apparent glenohumeral range includes scapular contribution. The accurate measurement requires the scapula to be stabilised against compensatory rotation throughout. A simple self-assessment: place the opposite hand on the shoulder being tested during the assessment and feel for the scapular movement that indicates compensation. If the shoulder blade moves toward the spine before the forearm reaches its end point, the scapula is compensating and true glenohumeral internal rotation is less than the apparent range.
The Horizontal Adduction Test
Horizontal adduction restriction (the cross-body stretch position) is a reliable predictor of posterior capsule tightness independent of internal rotation measurement. If bringing the arm across the body (horizontal adduction while the elbow points forward) feels tight or restricted before the forearm reaches the opposite shoulder, the posterior capsule is a significant restrictor. Many individuals with GIRD show horizontal adduction restriction before internal rotation restriction becomes symptomatic, making the horizontal adduction test a useful early screening tool.
When to Seek Assessment Before Self-Treating
Self-directed GIRD management through stretching is appropriate for mild to moderate internal rotation restriction without associated pain, crepitus, or neurological symptoms. Seek physiotherapist assessment before self-treating if: shoulder pain occurs during or after attempts at internal rotation stretching, sharp pain rather than stretch discomfort is the dominant sensation, symptoms are worsening despite 2 to 3 weeks of consistent stretching, or if there is a history of shoulder labral pathology, rotator cuff tear, or instability. These presentations may involve structural pathology that stretching alone cannot address and that aggressive posterior capsule stretching may worsen.
The 4 Most Effective Shoulder Internal Rotation Techniques
Technique Selection Based on Presentation
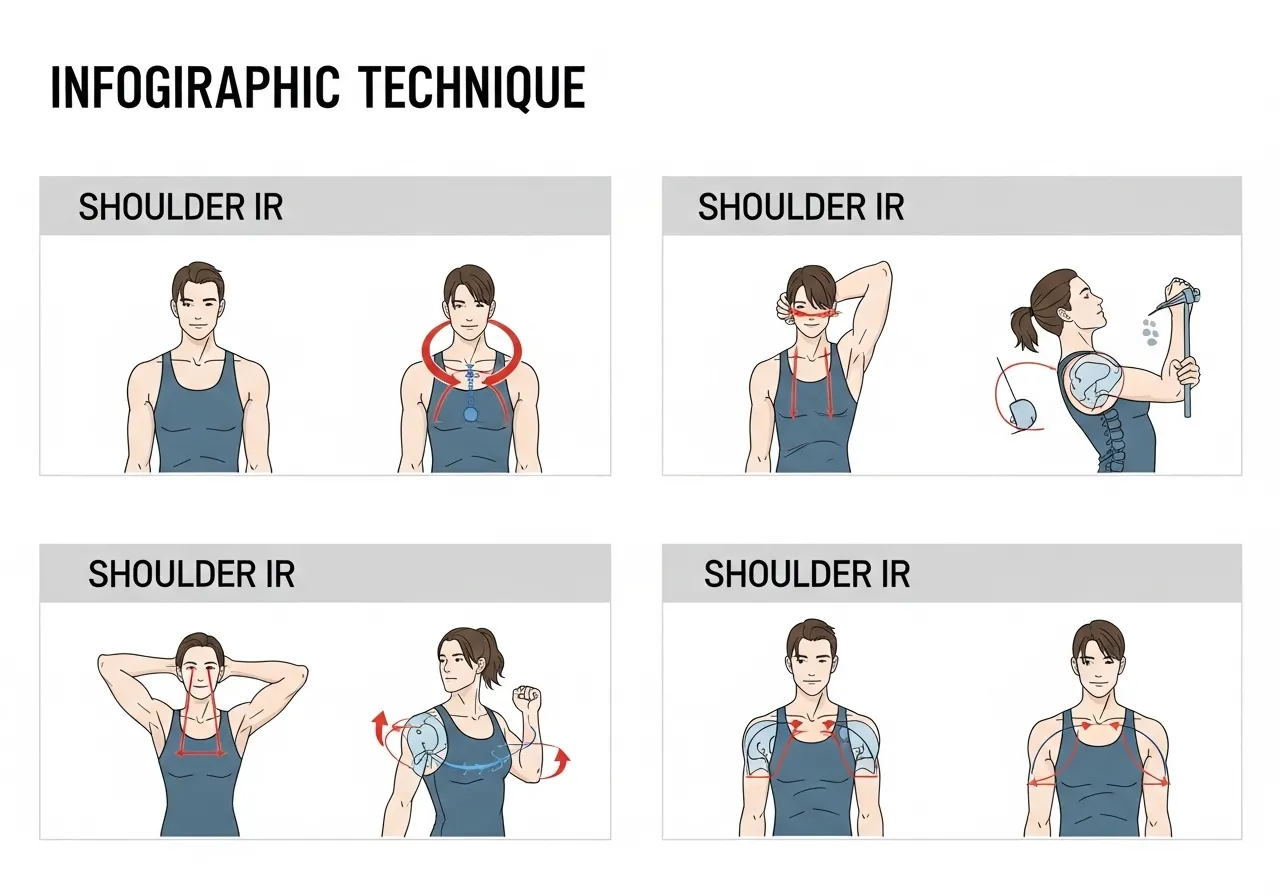
The four techniques below address different aspects of shoulder internal rotation restriction: posterior capsule lengthening through the side-lying position, posterior capsule and posterior rotator cuff combined stretch through horizontal adduction, active internal rotation restoration through muscle energy technique, and thoracic extension restoration that improves shoulder mechanics through improved scapular positioning. Most trainees benefit from combining at least two of these techniques rather than relying on a single approach.
🔄 1. Sleeper Stretch
Target: Posterior glenohumeral capsule, primary GIRD treatment for athletes
How: Lie on the side with the affected shoulder down. The shoulder should be at 90 degrees of abduction (upper arm parallel to the floor, perpendicular to the body). Bend the elbow to 90 degrees so the forearm points toward the ceiling. Using the opposite hand on the back of the forearm, gently press the forearm toward the floor (into internal rotation) until a mild stretch is felt deep in the posterior shoulder. Hold 30 seconds. Perform 3 repetitions.
Key point: Keep the shoulder stacked directly over the lower shoulder, not allowing the torso to roll backward. The shoulder must remain in 90 degrees of abduction throughout. If pain occurs in the anterior or superior shoulder, the abduction angle or the stretch force needs adjustment.
🔄 2. Cross-Body (Horizontal Adduction) Stretch
Target: Posterior capsule and posterior rotator cuff, generally more comfortable than sleeper stretch
How: Stand or sit upright. Bring the affected arm across the body at shoulder height, grasping the elbow with the opposite hand. Gently pull the arm further across the body until a stretch is felt in the posterior shoulder. Hold 30 seconds. Perform 3 repetitions.
Key point: Stabilise the scapula by slightly retracting the shoulder blade before applying the cross-body pull. If the shoulder blade wings forward during the stretch, reduce the pull and focus on maintaining the scapular position. This is the stretch that research suggests may be slightly more effective than the sleeper stretch for most individuals.
🔄 3. Passive Internal Rotation with Scapular Stabilisation
Target: Pure glenohumeral internal rotation with scapular compensation eliminated
How: Lie on the back. Abduct the shoulder to 90 degrees and bend the elbow to 90 degrees (forearm pointing to ceiling). Place the opposite hand on the front of the shoulder to stabilise the scapula against anterior rotation. Use the hand weight of the forearm or gentle opposite-hand pressure to internally rotate the shoulder passively toward the table. Hold the end range for 30 seconds without scapular movement. 3 repetitions.
Key point: The scapular stabilisation is the key feature that makes this stretch more specific to glenohumeral capsule than the unsupported sleeper or cross-body stretch, both of which allow scapular compensation that reduces the true glenohumeral stretch received.
🔄 4. Posterior Capsule Foam Rolling (Self-Myofascial Release)
Target: Posterior rotator cuff and capsule myofascial release before stretching
How: Position the foam roller or a massage ball against the posterior shoulder (the infraspinatus and teres minor region, below and medial to the posterior acromion). Apply body weight gently and slowly roll the roller or move the arm through internal and external rotation to mobilise the posterior soft tissue. Spend 60 to 90 seconds per side before performing the stretching techniques above.
Key point: Performing self-myofascial release before the stretching sequences reduces the posterior rotator cuff tension that limits the stretch depth, allowing greater range to be accessed during the subsequent stretching techniques. Research supports myofascial release as an adjunct to stretching for GIRD rather than a standalone intervention.
The 6-Week GIRD Restoration Protocol
Protocol Design Principles
Effective GIRD restoration requires daily consistency rather than high-volume sessions. The posterior capsule’s viscoelastic properties respond better to frequent, moderate-duration stretching than to infrequent long stretching sessions. Research on posterior capsule tissue mechanics confirms that daily stretching of 2 to 3 minutes per technique produces greater cumulative lengthening than three times weekly stretching of longer duration, because the tissue’s rebound to resting length between infrequent sessions partially negates the progress achieved.
📅 Phase 1: Weeks 1 to 2: Baseline Assessment and Gentle Introduction
- Posterior capsule foam rolling: 60 seconds each shoulder, daily
- Cross-body stretch: 3 × 30 seconds, twice daily (morning and evening)
- Assess internal rotation range before and after each session to track acute gains
- Do not force range — stretch should be felt as mild tension, not pain
Phase 1 establishes the stretching habit and identifies which technique produces the clearest posterior capsule sensation. Acute gains of 5 to 10 degrees per session confirm that the technique is accessing the posterior capsule correctly.
📅 Phase 2: Weeks 3 to 4: Progressive Loading and Technique Addition
- Add sleeper stretch: 3 × 30 seconds alongside cross-body stretch
- Add passive internal rotation with scapular stabilisation: 3 × 30 seconds
- Continue foam rolling before stretching sequence
- Measure internal rotation range weekly and compare to baseline
Expected Phase 2 progress: 10 to 20 degrees of internal rotation improvement from baseline in athletes. Non-athletes with postural restriction typically show greater improvement (20 to 30 degrees) because their restriction is primarily muscular and postural rather than structurally adaptive.
📅 Phase 3: Weeks 5 to 6: Thoracic Integration and Functional Restoration
- Maintain daily stretching sequence (reduced to once daily if progress is maintained)
- Add thoracic extension mobility work (foam roller thoracic extension, 2 minutes daily)
- Integrate restored internal rotation into overhead movement patterns
- Week 6: reassess internal rotation bilaterally versus Week 1 baseline
Phase 3 ensures restored passive range transfers to active functional range. Internal rotation improvements that remain passive but do not transfer to improved overhead mechanics indicate that scapular control or rotator cuff activation alongside the range restoration requires attention.
Maintenance After Restoration
Once the internal rotation deficit is corrected to within 18 degrees of the contralateral side (or within 10 degrees for non-athletes comparing bilateral sides), maintenance requires daily cross-body stretching for 60 to 90 seconds rather than the full therapeutic protocol. Athletes in high-volume overhead sports should perform this maintenance stretching after every training session as the posterior capsule will continue to tighten adaptively in response to eccentric throwing loads. The shoulder mobility comprehensive approach that addresses all ranges of shoulder motion is covered in the shoulder mobility guide.
Frequently Asked Questions About Shoulder Internal Rotation and GIRD
Can I stretch my shoulder internal rotation too aggressively?
Yes. Overly aggressive posterior capsule stretching, particularly the sleeper stretch when performed with excessive force or pain, can aggravate anterior shoulder structures including the bicep tendon and the anterior labrum. The stretch sensation should always be felt in the posterior shoulder — deep, mild, and diffuse. If the stretch produces anterior shoulder pain, sharp pain anywhere in the shoulder, or pain radiating down the arm, the technique is being applied incorrectly or there is underlying pathology that requires assessment before continuing. The common rule applies: stretch to mild tension, not to pain.
Why does my shoulder internal rotation keep getting tight even after I stretch it?
Persistent tightness despite regular stretching almost always indicates an ongoing mechanical cause that the stretching addresses temporarily but cannot resolve permanently. For overhead athletes, the cause is the ongoing eccentric loading of throwing and swinging that continuously stresses the posterior capsule. In this case, stretching is a maintenance tool rather than a cure, and reducing training volume during GIRD management periods may be necessary for meaningful structural change. For desk workers, the cause is the sustained sitting posture that continuously loads the posterior capsule in the same restricted position between stretching sessions. Addressing sitting posture and taking regular shoulder movement breaks prevents the posture from re-restricting the range that stretching restores.
Is GIRD always a problem that needs treating?
In overhead athletes, asymmetric GIRD (significant internal rotation loss on the dominant side) is associated with increased shoulder injury risk when the total rotation arc decreases. Isolated GIRD without total arc reduction, where internal rotation decreases by the same amount as external rotation increases, may be a normal adaptive finding rather than a pathological one that requires aggressive treatment. Symptomatic GIRD — where the internal rotation restriction is associated with shoulder pain during overhead movements — clearly warrants treatment. Asymptomatic GIRD in a non-overhead athlete without shoulder pain may not require dedicated treatment beyond maintaining adequate total arc of rotation and monitoring for symptom development.
How do I know if my shoulder internal rotation restriction is improving?
The most reliable indicator is a consistent measurement of internal rotation range of motion at the same position (90 degrees of shoulder abduction, 90 degrees of elbow flexion, supine with scapula stabilised) at the same time of day each week. Range measurements vary based on time of day and preceding activity, so consistency in measurement conditions is more important than achieving precise numbers. A sustained 10 to 15 degree improvement from baseline over 4 to 6 weeks of daily stretching confirms that the protocol is producing structural change rather than only acute viscoelastic effects that rebound between sessions.
Does strengthening matter alongside stretching for GIRD?
Yes, significantly. Stretching the posterior capsule and restoring passive internal rotation range addresses the mobility deficit but not the rotator cuff activation patterns that help maintain correct humeral head position during overhead movement. The infraspinatus and teres minor must be sufficiently active to hold the humeral head centred in the glenoid as it moves through the restored range. Without rotator cuff strengthening alongside capsule stretching, restored passive range may not translate to improved active overhead mechanics because the muscles responsible for using the new range lack the strength and activation patterns to do so reliably under loading. Incorporating external rotation strengthening (side-lying dumbbell external rotation, band pull-aparts, face pulls) alongside the GIRD stretching protocol produces more complete and durable functional restoration than stretching alone. The face pull and its role in rotator cuff and posterior shoulder strengthening alongside internal rotation restoration is covered in the face pull guide.
- Shoulder internal rotation deficit (GIRD) affects both overhead athletes (posterior capsule adaptive thickening) and desk workers (postural shortening), producing the same mechanical consequence: abnormal humeral head migration that compresses the supraspinatus during overhead movements.
- Both sleeper and cross-body stretches produce significant internal rotation improvements over 4 to 8 weeks. The cross-body stretch may be slightly more effective; patient comfort is a valid selection criterion. Consistent daily application matters more than which technique is chosen.
- Glenohumeral posterior mobilisation and sleeper stretches produce immediate internal rotation gains within a single session. Local shoulder interventions produce larger gains when performed before rather than after thoracic manipulation.
- A side-to-side internal rotation difference greater than 18 to 20 degrees in overhead athletes meets the clinical GIRD threshold and warrants a structured daily stretching programme. Asymptomatic GIRD in non-overhead athletes requires monitoring rather than aggressive treatment.
- Stretching alone is insufficient for complete GIRD management. External rotation strengthening alongside capsule stretching ensures restored passive range transfers to improved active overhead mechanics and maintained humeral head centring under load.











