Isometric training — holding a static contraction without joint movement — is one of the oldest forms of resistance exercise and one of the most under-appreciated in modern strength and conditioning. Its reputation as a limited, rehabilitation-only tool until two decades of research overturned that view that have established it as a genuinely effective intervention for blood pressure management, sport-specific strength development, and post-injury rehabilitation, each with a specific evidence base that positions isometric training as complementary to rather than merely a pale imitation of dynamic resistance exercise.
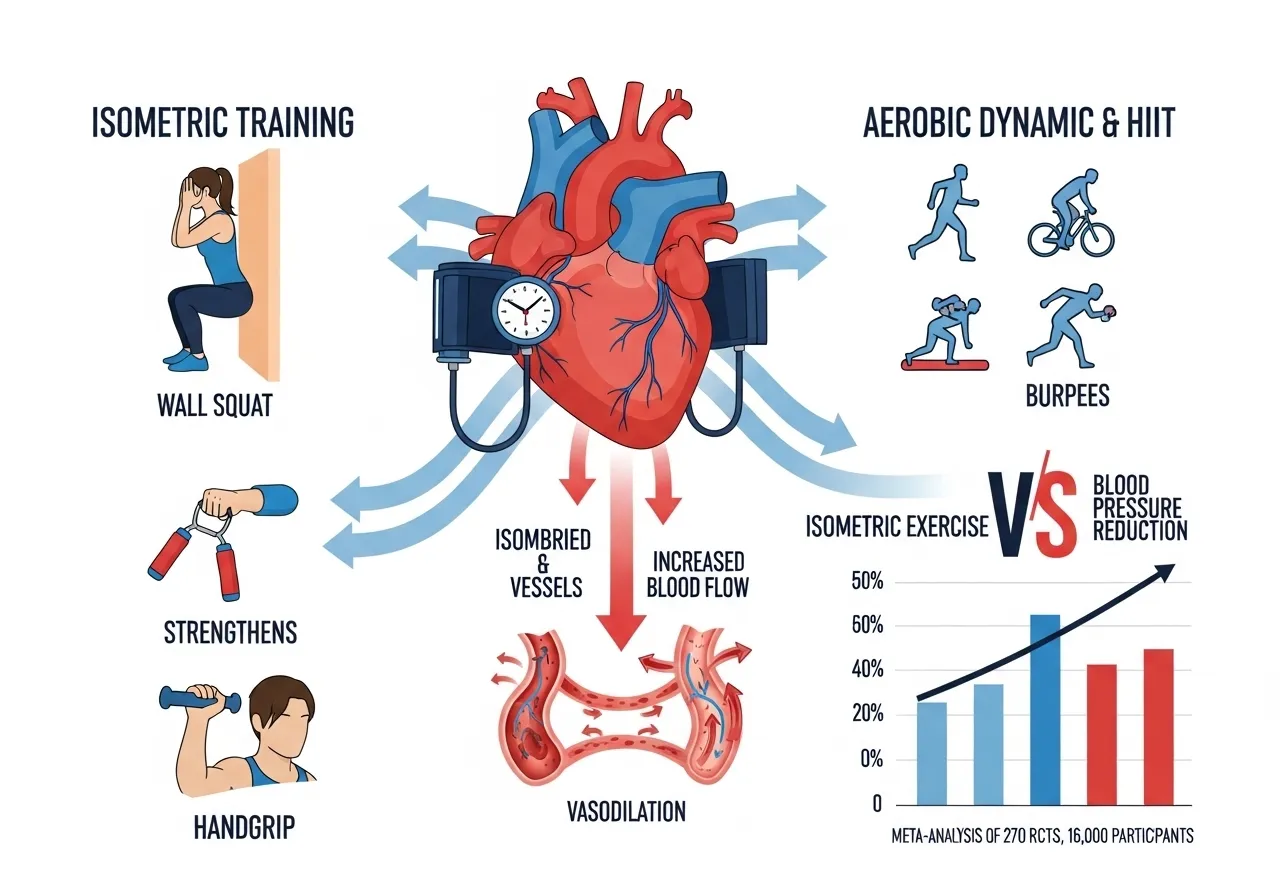
The blood pressure finding is the most striking: a 2023 meta-analysis of 270 randomised controlled trials covering nearly 16,000 participants found that isometric exercise was the most effective exercise mode for reducing blood pressure, outperforming aerobic exercise, dynamic resistance training, combined training, and HIIT. This is not a marginal difference but a clinically meaningful superiority that has prompted updated clinical guidance on exercise selection for hypertension management.
This guide covers the physiology of isometric contractions, what the research shows about isometric training for blood pressure, strength development, and rehabilitation, the diagnostic question of which training goal isometric training serves best, practical protocols for different applications, and how to integrate isometric work within a complete training programme.
Research 1: Isometric Training and Blood Pressure : The Superior Exercise Mode
The 2023 Meta-Analysis: Isometric Wins the Blood Pressure Exercise Comparison
📌 Key Finding
Isometric exercise training produces blood pressure reductions superior to aerobic exercise, dynamic resistance training, combined training, and HIIT. This positions isometric training as the most effective single exercise mode for blood pressure management based on the current RCT evidence base.
📌 Key Finding
IRT reduces systolic BP, diastolic BP, and mean arterial pressure across pre-hypertension to established hypertension. The blood pressure benefits are consistent across wall squat, leg extension isometrics, and handgrip modalities, confirming that multiple exercise forms deliver the blood pressure advantage.
📌 Key Finding
Isometric training is superior to HIIT for blood pressure reduction. HIIT is superior for overall cardiovascular conditioning and resting heart rate reduction. Both are complementary rather than competing tools in a complete cardiovascular health programme.
The Blood Pressure Mechanism: Why Static Contractions Lower BP
The mechanism by which isometric training reduces resting blood pressure involves sustained metabolic vasodilation during static contractions, post-exercise hypotension that is more pronounced after isometric than dynamic exercise at matched intensities, and chronic adaptations in endothelial function and arterial stiffness from repeated isometric training sessions. The sustained isometric contraction compresses the vasculature within the contracting muscle, triggering a reactive vasodilation response that temporarily lowers peripheral vascular resistance after the contraction releases. Repeated sessions of this ischaemia-reperfusion cycle in the contracting muscle produce chronic endothelial adaptations — improved nitric oxide signalling, reduced arterial stiffness — that lower resting blood pressure independently of exercise-session effects.
The Practical Implication: Low-Impact Blood Pressure Management
For hypertensive individuals who cannot tolerate high-impact cardiovascular exercise, or for older adults whose joint health limits running and cycling, isometric training’s blood pressure superiority over aerobic exercise at matched effort levels provides a meaningful clinical alternative. The wall squat, isometric leg press, and handgrip exercises that produce the strongest blood pressure reductions in the research require no special equipment, can be performed at home, and produce minimal joint impact — making them accessible to populations where the exercise modalities that have historically been first-line recommendations create barriers to participation.
Is Isometric Training Right for Your Goal? The Diagnostic Framework
Three Primary Applications: Blood Pressure, Strength, Rehabilitation
Isometric training’s effectiveness differs substantially across its three primary applications, and selecting it for the wrong goal produces disappointment that does not reflect the exercise’s genuine capabilities in its appropriate applications. Diagnosing which application applies to a specific trainee’s situation determines whether isometric training is the optimal primary tool, a valuable complementary tool, or an inappropriate choice relative to alternatives.
Application 1: Blood Pressure Management
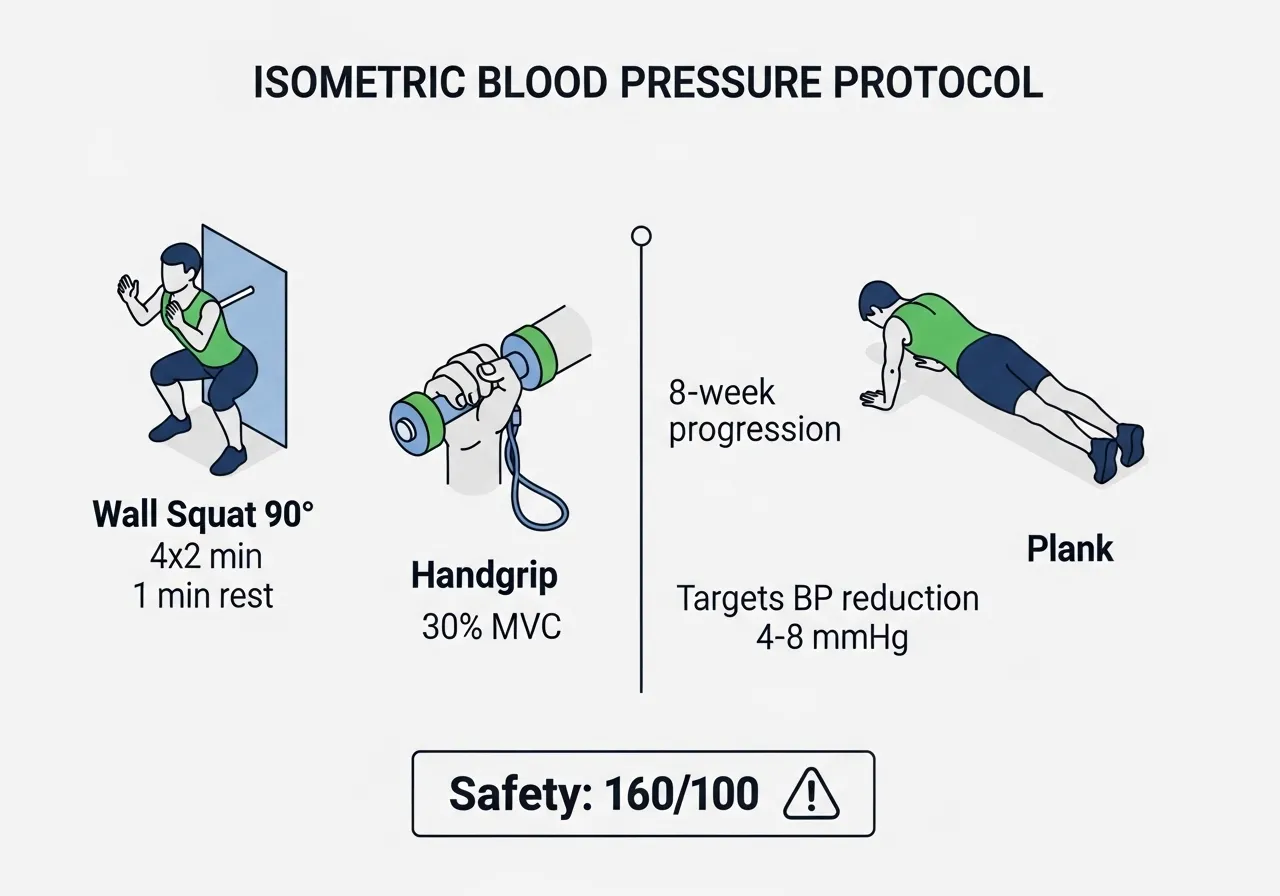
Isometric training is the optimal primary exercise tool for blood pressure management, based on the meta-analysis evidence reviewed above. The specific protocol that produces the strongest blood pressure evidence is the wall squat: sustained isometric quadriceps and glute contraction at 90 to 120 degrees of knee flexion for 2 minutes, repeated 4 times with 1-minute rest between contractions, 3 sessions per week for 4 to 8 weeks. Isometric handgrip training at 30% maximum voluntary contraction for 2-minute holds is the alternative protocol with comparable evidence for individuals who cannot perform the wall squat due to knee pain or limited lower body capacity.
Application 2: Specific Strength at a Specific Joint Angle
Isometric training develops strength at and near the specific joint angle at which the contraction occurs, with limited carryover to other angles in the same movement. This angular specificity makes isometric training the optimal tool for addressing a specific sticking point in a dynamic lift — the position in a squat, bench press, or deadlift where the bar slows or stops. Isometric training at the specific sticking-point angle develops the maximal force production capacity at that angle more directly than any dynamic exercise that passes through the angle briefly during a full-range movement.
This application is appropriate for intermediate and advanced strength athletes who have identified a specific angular weakness rather than a general strength deficit. The contrast training and post-activation potentiation principles that complement isometric sticking-point training are covered in the contrast training guide.
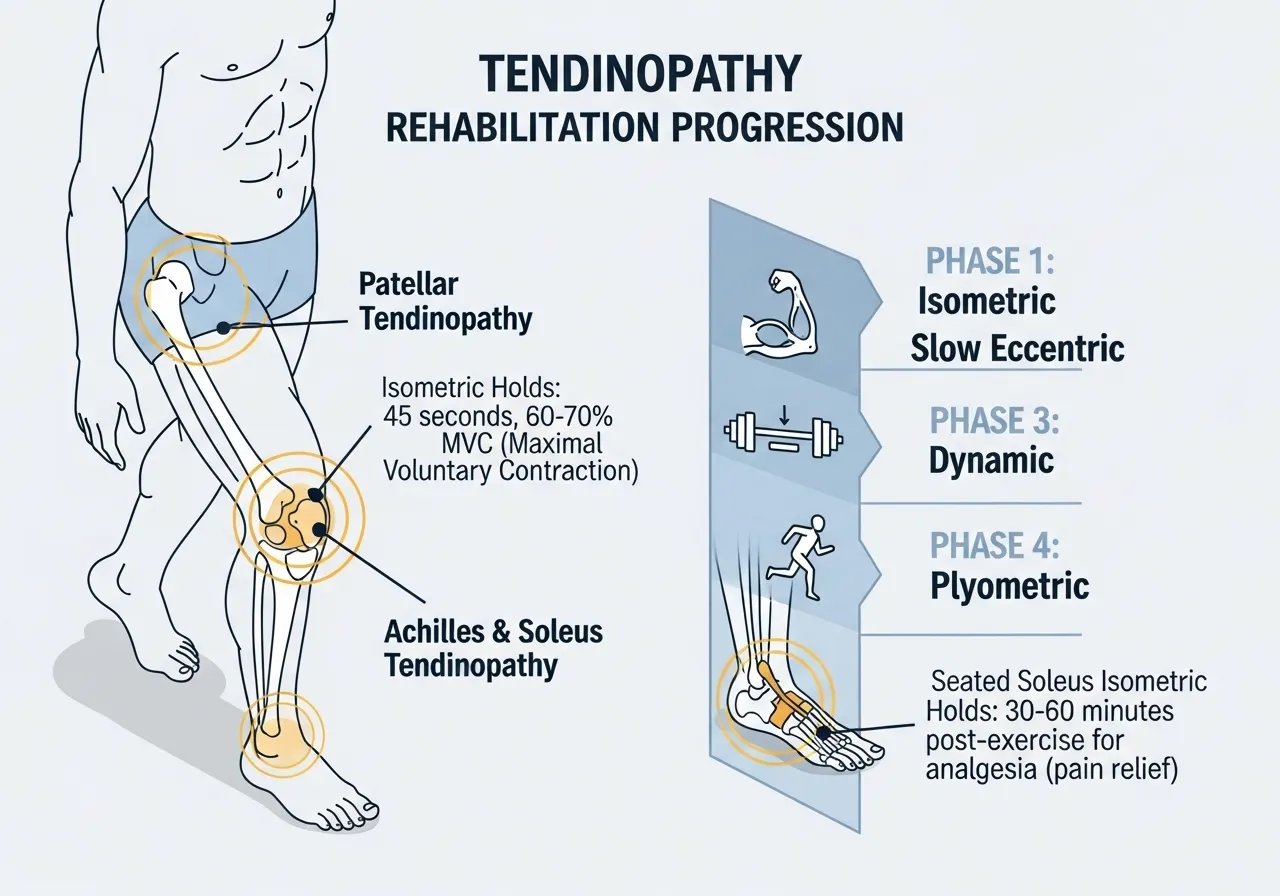
Application 3: Rehabilitation and Tendon Loading
Isometric training is the evidence-based first-line treatment for tendinopathy rehabilitation, particularly patellar tendinopathy and Achilles tendinopathy. The key property is that isometric contractions load the tendon without the cyclic compression that dynamic exercises produce at the same joint, which is important because tendons with active pathology are more sensitive to cyclic compressive loading than to sustained isometric tension. Isometric quadriceps contractions at 60 to 70% maximum voluntary contraction for 45-second holds, performed 5 repetitions with 2-minute rest, are the protocol with the strongest patellar tendinopathy rehabilitation evidence.
When Isometric Training Is Not the Right Tool
Isometric training does not develop the dynamic strength through full range of motion, muscle hypertrophy, or power output that dynamic resistance training provides. For trainees whose primary goal is overall strength development, muscle hypertrophy, or athletic power expression, dynamic resistance training is the appropriate primary tool and isometric work is supplementary. The angular specificity of isometric strength gains also means that isometric training alone produces strength that does not transfer broadly to dynamic performance — a trainee who primarily performs isometric squats does not develop the same dynamic squat strength as one who performs dynamic loaded squats, even if their isometric squat force at a given angle is high.
The Self-Assessment: Which Application Applies to You?
Ask three questions. First, is blood pressure management a training goal? If yes, isometric training is primary. Second, do you have a specific sticking point in a compound lift that limits performance despite general strength adequacy? If yes, targeted isometric training at the sticking-point angle is a valuable supplementary tool. Third, do you have a tendinopathy diagnosis (patellar, Achilles, or proximal hamstring) that is limiting dynamic loading? If yes, isometric rehabilitation loading is the evidence-based first intervention before progressive dynamic loading is reintroduced. If none of these apply, isometric training is a supplementary tool that provides variety and joint-angle-specific stimulus alongside primary dynamic training.
Blood Pressure Protocol: The Evidence-Based Wall Squat and Handgrip Programme
The Wall Squat Protocol
The wall squat is the single best-evidenced isometric exercise for blood pressure reduction based on the volume of RCT research supporting it. The protocol requires no equipment beyond a smooth wall, can be performed at home, and produces blood pressure reductions within 4 weeks of three-sessions-per-week practice.
🏋️ Wall Squat Protocol
Position: Back flat against the wall, feet hip-width and approximately 60 to 70 cm from the wall. Slide down until the thighs are approximately parallel to the floor (90 to 120 degrees of knee flexion). Maintain this position with back contact against the wall throughout.
Dosage: 4 repetitions of 2-minute holds, with 1-minute rest between each hold. Total active work time: 8 minutes per session.
Frequency: 3 sessions per week, non-consecutive days. Minimum 8 weeks for blood pressure adaptation.
Intensity: The hold should feel moderately challenging in the quadriceps and glutes — not easy, but sustainable for the full 2 minutes. If the hold cannot be sustained for 2 minutes, reduce the knee flexion angle (higher position) until 2 minutes is achievable, then progressively lower the position over weeks.
The Handgrip Isometric Protocol
Handgrip isometric training is the alternative protocol for individuals with knee pathology that prevents the wall squat, or as a complementary addition to the wall squat programme.
🏋️ Handgrip Protocol
Equipment: A handgrip dynamometer or a firm rubber ball that provides measurable resistance. A maximum voluntary contraction (MVC) test must be performed first to determine the 30% target — the typical handgrip MVC for an adult male is 40 to 55 kg, so 30% is approximately 12 to 17 kg of grip force.
Dosage: 4 repetitions of 2-minute holds per hand, alternating hands with 1-minute rest between holds.
Frequency: 3 sessions per week. 8 to 10 weeks for measurable blood pressure reduction.
Limitation: Handgrip dynamometers are not standard gym equipment. A firm rubber ball, gripped at the effort level that feels like 30% of maximum squeeze, provides a practical alternative for home use without measurement.
The Plank for Core and Blood Pressure
The forearm plank, performed as a 2-minute sustained hold at 3 to 4 repetitions with 1-minute rest, provides both the core deep stabilisation stimulus covered in the deep core training research and the isometric blood pressure benefit in a single exercise. Research on plank isometric training confirms blood pressure reductions consistent with other isometric modalities, with the additional benefit of core stabilisation development that the wall squat and handgrip do not provide. The deep core and TVA activation that the plank develops alongside its blood pressure benefit is covered in the deep core training guide.
Progression Over 8 Weeks
📅 8-Week Blood Pressure Isometric Programme
Weeks 1 to 2: Wall squat 4 × 90 seconds (build to 2 minutes), 3 days per week
Weeks 3 to 4: Wall squat 4 × 2 minutes + handgrip 2 × 2 minutes per hand
Weeks 7 to 8: Full protocol at established dosages, monitor BP weekly
Target: 4 to 8 mmHg reduction in systolic BP, 2 to 4 mmHg diastolic reduction
These are the blood pressure reductions documented in the research literature at 8 weeks. Individual responses vary. Blood pressure should be measured on a rest day in the morning before other activity for the most consistent tracking.
Safety Considerations for Blood Pressure Isometric Training
Isometric contractions produce acute blood pressure elevations during the hold that return to below-resting levels in the post-exercise recovery period, ultimately producing chronic resting BP reduction. This acute elevation is the mechanism that drives chronic adaptation. For individuals with very high resting blood pressure (above 160/100 mmHg), medical clearance before beginning isometric training is appropriate because the acute elevation during holds may be significant. For individuals with controlled or mild to moderate hypertension (below 160/100 mmHg) who are already cleared for exercise by their physician, isometric training as described is appropriate and evidence-supported.
Strength and Sticking-Point Protocol: Using Isometrics for Performance
The Sticking Point Problem in Strength Training
Most compound lifts have a specific angular range where the mechanical disadvantage is greatest — where the moment arm between the barbell and the joint is longest relative to the muscles’ capacity to produce torque. For the squat, this is typically at 90 degrees of knee flexion where the quad’s mechanical advantage is reduced. For the bench press, this is typically at 90 degrees of elbow flexion, mid-range. For the deadlift, this is typically just above the floor, where the back extensor moment arm is longest relative to the hips.
Isometric training at the specific sticking-point angle develops force production capacity at exactly the position where the dynamic lift fails. This is more direct than dynamic exercise that passes through the sticking point briefly and relies on the momentum from the earlier range to carry the load through the angle of greatest difficulty.
Overcoming Isometrics: Maximum Force Against a Fixed Object
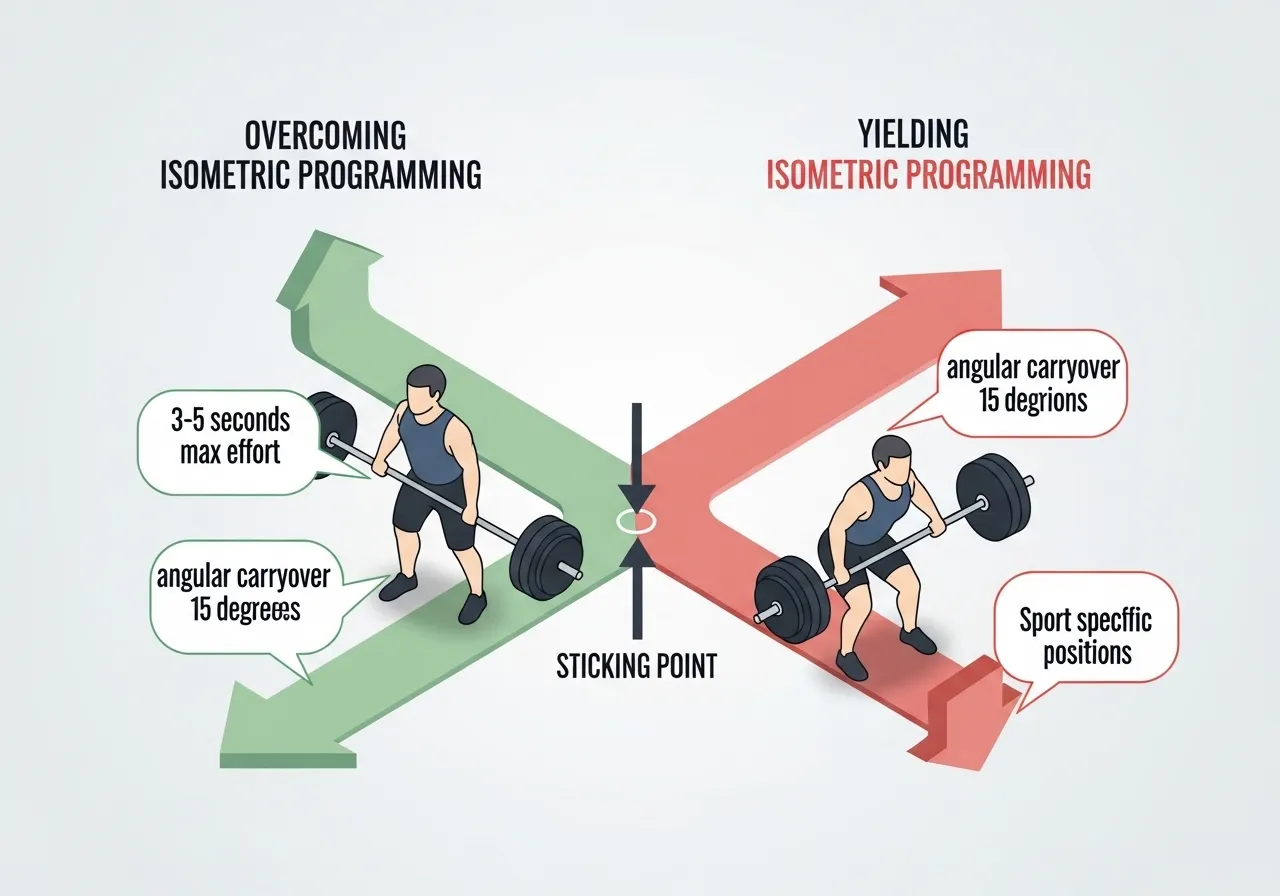
Overcoming isometrics — pushing or pulling with maximum force against an immovable resistance — are the most potent isometric training stimulus for strength development. Setting a safety bar at the sticking-point angle in a squat rack and pushing upward against it with maximum force for 3 to 6 seconds produces peak neural drive at the specific angle that constitutes a squatter’s sticking point. Research on overcoming isometrics confirms force production that exceeds what can be achieved with any loaded barbell movement because there is no deceleration phase, no concern about the bar moving too fast, and no upper limit imposed by the loaded weight — only the maximum force the nervous system can produce against an immovable resistance.
Yielding Isometrics: Holding a Load at Angle
Yielding isometrics — holding a loaded position against resistance at the target angle — provide a less maximal but more accessible sticking-point training tool that does not require a power rack with adjustable safety bars. Holding a loaded barbell in the bottom position of a squat for 3 to 5 seconds, or pausing a bench press at the sticking point angle, are yielding isometric applications that can be integrated into standard strength training sessions without additional equipment setup.
Programming Sticking-Point Isometrics
Two to three sets of overcoming isometrics at the sticking-point angle, performed at maximum voluntary effort for 3 to 5 seconds per repetition with 2 to 3 minutes rest, performed twice weekly, produces measurable sticking-point strength improvement within 3 to 4 weeks. The isometric training produces force production improvements at and near the trained angle that transfer to improved dynamic lift performance through the sticking point. The angular carryover is approximately plus or minus 15 degrees from the trained angle, so precise identification of the sticking-point angle is important for targeted training. The trap bar deadlift’s force-time characteristics at different positions in the pull, which inform sticking-point identification for hip hinge movements, is covered in the trap bar deadlift guide.
Functional Isometrics for Sport
Many sport-specific positions require sustained force production without joint movement — a rugby scrum, a wrestling hold, a swimming push-off. Isometric training in the sport-specific position develops the force production capacity and muscular endurance that dynamic resistance exercises performed in different positions cannot directly replicate. Sport-specific isometric training for these applications uses the sport position as the trained angle and develops holding strength and force production capacity in exactly the mechanical condition that the sport demands.
Rehabilitation Protocol: Isometrics for Tendinopathy and Post-Injury Recovery
Why Tendons Respond Differently to Isometric vs Dynamic Loading
Tendons respond to mechanical loading by increasing collagen synthesis and reorganisation in the direction of the applied load. The research on tendinopathy rehabilitation has established that the loading pattern matters as much as the loading magnitude: cyclic compressive and tensile loading at high velocities (as in plyometrics and fast dynamic exercise) can aggravate tendon pathology, while sustained isometric loading provides the tensile stimulus for collagen synthesis without the compression and velocity components that provoke reactive tendinopathy.
This distinction makes isometric loading the first-stage rehabilitation intervention for reactive tendinopathies. The isometric contraction loads the tendon through the muscle’s pull without joint movement that creates compression at the tendon’s insertion or the velocity loading that provokes reactive tissue response. Starting the rehabilitation load-building process with isometrics before progressing to dynamic loading respects the tendon’s tissue state and accelerates recovery compared to returning immediately to dynamic loading that re-aggravates the reactive tissue.
Patellar Tendinopathy: The 45-Second Hold Protocol
🏋️ Isometric Patellar Tendon Loading Protocol
Position: Leg extension machine at 60 degrees of knee flexion, or wall squat at 60 degrees knee flexion. Both positions load the patellar tendon isometrically without compression at the tendon insertion.
Dosage: 5 repetitions of 45-second holds at 60 to 70% maximum voluntary contraction, with 2-minute rest between holds. Daily or twice daily during the acute-to-subacute rehabilitation phase.
Expected effect: Immediate pain reduction lasting 45 to 60 minutes post-exercise (the isometric analgesia effect), and progressive tendon load tolerance development over 4 to 6 weeks of consistent application.
Achilles Tendinopathy: Seated Calf Isometrics
🏋️ Isometric Achilles Loading Protocol
Position: Seated with the knee bent to 90 degrees (isolating the soleus component of the Achilles). Press the foot into a fixed platform at 60 to 70% maximum voluntary plantarflexion force.
Dosage: 5 repetitions of 45-second holds with 2-minute rest. Daily during the acute phase, reducing to 3 times weekly as symptoms improve and dynamic loading is reintroduced.
Key point: The seated (knee bent) position specifically loads the soleus and the mid-portion of the Achilles. Insertional Achilles tendinopathy (at the heel bone) requires modified positioning to avoid the compression that the isometric position otherwise produces at the insertion.
The Isometric Analgesia Effect
One of the most useful practical properties of isometric loading in tendinopathy is the immediate pain reduction it produces for 30 to 60 minutes after the session, through a mechanism involving central pain modulation rather than direct tendon changes. This post-isometric analgesia allows athletes with tendinopathy to participate in sport or training sessions with reduced pain by timing their isometric loading protocol 30 to 60 minutes before the athletic activity. The pain reduction is not a sign that the tendon is healing faster but a central modulation effect that makes the athletic session more manageable during the rehabilitation period.
Progressing From Isometric to Dynamic Loading in Rehabilitation
The rehabilitation progression for tendinopathy moves from isometric to isotonic (slow dynamic) to dynamic loading in stages, advancing each stage only when the previous stage is tolerated without symptom aggravation. Typical progression: isometric for 4 to 6 weeks, slow eccentric for 4 to 6 weeks, full dynamic loading for 4 to 6 weeks, then plyometric loading for athletic populations in the final rehabilitation stage. Isometric training’s role is specifically in the first stage of this progression, not as a long-term rehabilitation tool that replaces dynamic loading indefinitely.
Frequently Asked Questions About Isometric Training
Does isometric training build muscle?
Isometric training at sufficient intensity (above 60 to 70% maximum voluntary contraction) produces muscle hypertrophy in the trained muscle, but the hypertrophy is more limited and angular-specific than dynamic resistance training at matched volumes. The time under tension during isometric holds is theoretically favourable for hypertrophy, but the absence of a full range of motion means the muscle is not trained through the length changes that dynamic exercise develops. For muscle hypertrophy as a primary goal, dynamic resistance training is superior. Isometric training at high intensities produces measurable but limited hypertrophy as a secondary benefit to its primary applications in blood pressure management, sticking-point strength, and tendinopathy rehabilitation.
Is isometric training safe for older adults?
Isometric training is particularly well-suited to older adults for three reasons: it requires no dynamic joint loading that could aggravate arthritic joints, the exercise can be performed at home without equipment for the blood pressure protocol, and it produces blood pressure and functional strength improvements relevant to the primary cardiovascular and musculoskeletal health concerns of ageing. The wall squat and handgrip protocols are commonly used in older adult exercise interventions specifically because of their safety profile — the load is entirely body weight or grip force, there is no external weight to manage, and there is no falling risk during the exercise.
The acute blood pressure elevation during isometric holds warrants attention in older adults with very high resting blood pressure: medical clearance before beginning any exercise programme, including isometric training, is appropriate for this population as it would be for any exercise prescription.
How does isometric training compare to yoga and pilates for strength and blood pressure?
Yoga and pilates include many isometric contraction components within their practice — held postures in yoga and sustained core activation in Pilates are isometric in nature. However, the intensity of these isometric contractions is typically below the 40 to 60% maximum voluntary contraction threshold that the blood pressure and strength research uses for its effective protocols. The wall squat at 90 degrees, performed at 60 to 70% MVC, is a significantly higher intensity isometric stimulus than most yoga or Pilates holds at the same joint angle.
This does not make yoga or Pilates ineffective — they provide flexibility, coordination, and postural stability benefits that standard isometric training does not. But for the specific blood pressure and sticking-point strength applications where isometric training is most effective, the intensity of the specific research protocols is required, and yoga or Pilates alone do not reliably deliver that intensity threshold.
Can I combine isometric training with my regular strength programme?
Yes, and this is the appropriate use of isometric training for most recreational athletes and strength trainees. Blood pressure protocols (wall squat, handgrip, plank) require only 10 to 15 minutes and can be performed on rest days or at the end of regular training sessions without significant fatigue interference. Sticking-point overcoming isometrics can be programmed as a warm-up for the specific compound lift they target, performed at maximum effort for 3 to 5 seconds per repetition before the dynamic lift, using the post-activation potentiation mechanism to enhance the subsequent dynamic performance. Rehabilitation isometrics are performed as a standalone protocol, typically daily, separately from the main training session during the acute tendinopathy phase.
How quickly does isometric training reduce blood pressure?
Research on isometric training and blood pressure consistently documents measurable reductions in resting systolic blood pressure within 4 weeks of three-sessions-per-week practice, with clinically meaningful reductions of 4 to 8 mmHg systolic at 8 weeks. This timeline is comparable to or faster than the blood pressure reductions from aerobic exercise training at equivalent session frequency. The blood pressure reductions persist for as long as the training is maintained and regress toward baseline values within 4 to 6 weeks of stopping, which means isometric training for blood pressure requires long-term maintenance rather than a single programme completion.
Key Takeaways
Isometric exercise training produces blood pressure reductions superior to aerobic exercise, dynamic resistance training, combined training, and HIIT in meta-analysis comparison. It is the most effective single exercise mode for blood pressure reduction in the current RCT evidence base.
The wall squat protocol (4 × 2-minute holds, 3 days per week, 8 weeks) is the best-evidenced blood pressure isometric intervention. Handgrip isometrics at 30% MVC provide an equivalent alternative for those who cannot perform the wall squat.
Isometric training develops strength at and near the specific trained joint angle, making it the optimal tool for sticking-point strength development in compound lifts rather than general strength building across the full range.
Isometric loading is the evidence-based first-stage intervention for reactive tendinopathies, providing the tensile tendon load for collagen synthesis without the cyclic compression that dynamic exercise applies at the same load.
Isometric training complements rather than replaces dynamic resistance training and cardiovascular exercise. Its primary value is in the specific applications where its unique mechanical properties produce outcomes that dynamic exercise cannot match — blood pressure management, sticking-point strength, and tendinopathy rehabilitation.
Most athletic training focuses on going faster: building power for acceleration, developing explosive force for jumping, increasing speed across distances. Training to slow down receives a fraction of this attention, despite the fact that most non-contact ACL injuries occur during deceleration, not acceleration. Deceleration is the act of rapidly reducing speed during running, landing, or…
The farmer’s walk may be the most honest exercise in strength training. You pick up something heavy in each hand, walk until you cannot continue, and put it down. There is no technique to hide behind, no momentum to exploit, and no machine to stabilise the load. If the grip fails, the set ends. If…
Most training programmes develop either strength or power. Powerlifters squat heavy and get strong. Sprinters sprint fast and get explosive. The two qualities rarely develop in the same session, in the same set pairing, or even in the same training block. Contrast training challenges this separation. By pairing a heavy compound lift with an explosive…
Battle ropes sit in most gyms but get used by a minority of members. The exercise looks unusual — swinging heavy ropes in wave patterns doesn’t resemble any conventional cardiovascular or strength exercise — and its place in a training programme is less obvious than a treadmill interval or a barbell lift. The research tells…
⚠️ Health & Fitness DisclaimerThis article is for general educational purposes only and does not replace professional medical advice. If you have any lower limb, knee, or ankle conditions, please consult a qualified healthcare professional before beginning plyometric training overview training. Plyometric training — exercise that uses the stretch-shortening cycle (the rapid lengthening of a…
⚠️ Fitness Disclaimer: The information in this article is for general educational purposes only and does not constitute professional fitness or medical advice. Always consult a qualified healthcare professional before starting any new exercise program, especially if you have existing injuries or medical conditions. The Ball That Made My Conventional Training Feel Incomplete I added…






")





